This is an automatically translated article.
Posted by Master, Doctor Mai Vien Phuong - Gastrointestinal Endoscopy - Department of Medical Examination & Internal Medicine - Vinmec Central Park International HospitalProton Transfer Reaction-Mass Spectrometry is a method of using breath to check patients for esophageal cancer.
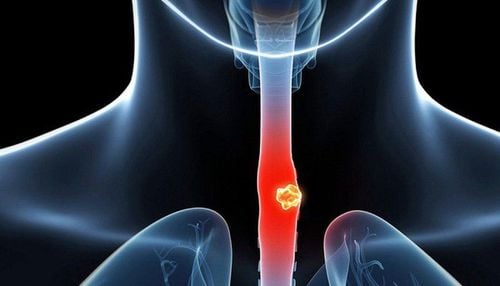
1 Overview of esophageal cancer
Esophageal cancer is the sixth leading cause of cancer death worldwide. Histologically, it is classified into 2 subtypes, squamous cell carcinoma and adenocarcinoma, each with a specific cellular origin, pathogenesis, and epidemiology.The current gold standard techniques for detecting and diagnosing esophageal cancer are endoscopic and biopsy is invasive. Furthermore, due to the absence of symptoms at earlier disease stages, presentation and diagnosis are often late, resulting in a poor prognosis and 5-year survival rates as low as 15%. Early diagnosis is associated with a much higher 5-year survival rate, and when limited to mucosal disease, specific survival rates of up to 98% have been reported.
Better diagnostic methods are needed to move the majority of diagnoses to the earliest stages and expand access to routine esophagoscopy and wider use in the setting of ineffective screening cost results. Minimal and noninvasive biomarkers, mainly in blood and breath, represent the most likely candidates to facilitate early detection of esophageal cancer.
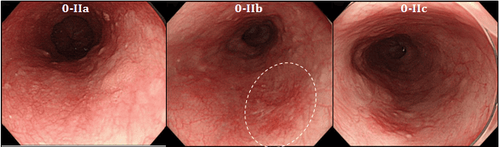
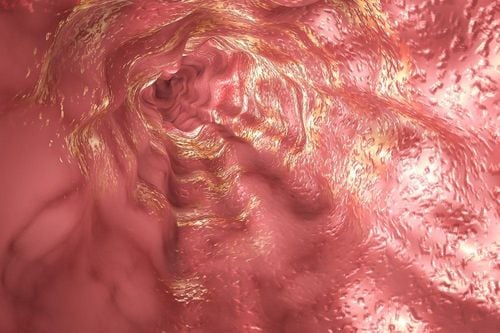
Ung thư thực quản giai đoạn sớm được nhìn thấy qua nội soi
2 What are biomarkers?
Several candidate biomarkers for esophageal cancer have been proposed. However, their translation into clinical use has been slow. Biomarkers can be broadly defined as quantifiable parameters that differentiate normal processes from pathological ones with applications for diagnosis, prognosis, and treatment adjustment of patients. In this article, we summarize recent insights into the development and clinical validation of esophageal cancer biomarkers. Since an important group of studies has been performed evaluating tissue-based biomarkers in esophageal cancer, this review has intentionally focused on minimally invasive and non-invasive methods for the detection of esophageal cancer. oesophageal cancer, markers circulating mainly in the blood and emerging areas of the breath and odor biomarkers. The development of powerful, minimally invasive, cost-effective biomarkers for early cancer will change current diagnostic, prognostic, and surveillance models and may open up possibilities population screening.
Dấu ấn sinh học ngày càng được sử dụng nhiều trong chẩn đoán bệnh ung thư
3. Current diagnostic methods of esophageal cancer
The diagnosis of esophageal cancer and its premalignant lesions is currently limited to endoscopy and subsequent biopsy analysis. Endoscopy is a highly invasive and expensive diagnostic procedure and the current gold standard diagnostic technique for esophageal cancer and its precancerous lesions. Standard white light endoscopy is limited in its scope, limited to identifying macroscopic abnormalities that may indicate cancer, such as nodules and ulcers, and therefore cannot identify Early lesions appear to be grossly normal. While Barrett's esophagus is visible endoscopically, dysplasia in the Barrett segment is more difficult to identify because the lesions are often flat and difficult to distinguish from the surrounding non-dysplastic columnar epithelium.Endoscopic surveillance and biopsy are often recommended for patients with Barrett's esophagus, to diagnose esophageal cancer in its earliest stages. Because of the low rate of progression of early lesions, such as Barrett's esophagus to adenocarcinoma, and the cost of endoscopic follow-up, the application of current diagnostic procedures in cancer surveillance Esophageal cancer may not be effective, and screening programs have never been considered viable. Therefore, there is an urgent need for the development of more selective and less invasive diagnostic techniques for individuals at risk for esophageal cancer.
Currently, screening for gastrointestinal cancer is a scientific and effective measure for early detection of gastrointestinal cancer (esophageal cancer, stomach cancer, colon cancer) and giving a treatment plan. best treatment. Currently, Vinmec International General Hospital has a package of screening and early detection of cancers of the gastrointestinal tract (esophagus - stomach - colon) combined with clinical and paraclinical examination to bring the most accurate results. maybe.

Hiện nay, khám sàng lọc ung thư đường tiêu hoá là biện pháp khoa học và hiệu quả để phát hiện sớm ung thư đường tiêu hóa
Gastrointestinal examination with an oncologist (by appointment). Gastroscopy and colonoscopy with an NBI endoscope with anesthesia. Peripheral blood count (laser counter). Automated prothrombin time test. Automated thrombin time test. Activated Partial Thromboplastin Time (APTT) test using an automated machine. General abdominal ultrasound
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
References1. Pakzad R , Mohammadian-Hafshejani A, Khosravi B, Soltani S, Pakzad I, Mohammadian M, Salehiniya H, Momenimovahed Z. The incidence and mortality of esophageal cancer and their relationship to development in Asia. Ann Transl Med. 2016; 4:29. [PubMed] [DOI]
2. Bystricky B , Okines AF, Cunningham D. Optimal therapeutic strategies for resectable oesophageal or oesophagogastric junction cancer. Drugs. 2011; 71 :541-555. [PubMed] [DOI]
3. Bandla S, Pennathur A, Luketich JD, Beer DG, Lin L, Bass AJ, Godfrey TE, Little VR. Comparative genomics of esophageal adenocarcinoma and squamous cell carcinoma. Ann Thorac Surg. 2012; 93 :101-1106. [PubMed] [DOI]
4. Bird-Lieberman EL, Fitzgerald RC. Early diagnosis of oesophageal cancer. Br J Cancer. 2009; 101 :1-6. [PubMed] [DOI]
5. Yentz S, Wang TD. Molecular imaging for guiding oncologic prognosis and therapy in esophageal adenocarcinoma. Hosp Pract (1995). 2011; 39 :97-106. [PubMed] [DOI]
6. Jankowski J , Barr H, Wang K, Delaney B. Diagnosis and management of Barrett's oesophagus. BMJ. 2010; 341 :c4551. [PubMed] [DOI]
7. Roger Yazbeck, Simone E Jaenisch, David I Watson. From blood to breath: New horizons for esophageal cancer biomarkers, World J Gastroenterol. Dec 14, 2016; 22(46): 10077-10083.