This is an automatically translated article.
Posted by Master, Doctor Mai Vien Phuong - Gastrointestinal Endoscopy - Department of Medical Examination & Internal Medicine - Vinmec Central Park International HospitalThe demand for more effective methods of detecting early esophageal cancer features has led to intensive research in the field of artificial intelligence (AI). Deep learning (DL) has brought about breakthroughs in image, video and other aspects of processing, while complex neural networks (CNNs) have paved the way for detect high-resolution endoscopic images and videos.
1. The role of artificial intelligence AI in early detection of esophageal cancer
1.1 Barrett's dysplasia and early-stage esophageal adenocarcinoma Artificial intelligence AI based on white light endoscopy (WLE) and NBI narrowband endoscopy : There are some limitations to recognition of early cancerous lesions associated with Barrett's esophagus using WLE, a common technology. High-definition WLE (HD-WLE) and the NBI endoscopic system were once considered to improve the accuracy of diagnosing early cancerous lesions associated with Barrett's esophagus, but improvement has not yet resulted. satisfied endoscopists. This situation stimulated the development of a CAD system for early cancerous lesions in Barrett's esophagus based on a supervised ML blood learning algorithm.1.2 Role of endoscopic coherence optical tomography (EOCT) and endoscopic confocal laser (CLE) AI Artificial Intelligence based on endoscopic optical tomography and confocal laser endoscopy: Beyond WLE and NBI, endoscopic coherent optical tomography (EOCT) and endoscopic confocal laser (CLE) techniques are also used for early diagnosis of EAC/BE-associated dysplasia. EOCT can identify early tumor lesions associated with Barrett's esophagus by analyzing mucosal and submucosal structures of the esophagus. CLE can observe mucosal tissue and cell morphology to achieve optical biopsies. However, the complexity of these two imaging technologies, the time-consuming reading of the images, and the requirement of a senior endoscopist have limited their clinical use. To solve this problem, Qi et al extracted multiple EOCT imaging features and combined one or more features to classify lesions, but the results were not satisfactory. Then, Swager et al used volumetric laser endoscopic imaging (VLE, integrated with 2nd generation OCT) for training and testing, and the results showed that the CAD system was superior to VLE experts.
1.3 Esophageal squamous dysplasia and early-stage esophageal squamous cell carcinoma AI-based WLE and NBI: Lugol's pigment endoscopy is the standard screening method for squamous cell carcinoma Esophageal; however, due to low specificity and long duration of consumption, new endoscopic techniques are required. Although WLE has been shown to be unsuitable for early esophageal squamous cell carcinoma screening alone, given its clinical prevalence, some researchers still hope to introduce AI to improve the accuracy of WLE.

Yêu cầu về các phương pháp phát hiện các đặc điểm ung thư thực quản sớm hiệu quả hơn đã dẫn đến các nghiên cứu chuyên sâu trong lĩnh vực trí tuệ nhân tạo (AI)
2. The role of artificial intelligence AI in endoscopy (endoscopy at the cellular level)
Artificial intelligence AI based on high resolution endoscopy and microscopic endoscopy: Endoscopic endoscopy (endoscopy at the cellular level) is a new technology that combines magnified endoscopy with staining importance. Due to the excellent magnification, the endoscope can clearly visualize the epithelial cells of the esophageal mucosa to achieve an effect similar to the diagnosis of pathology.If endoscopists want to use endoscopes to independently complete real-time detection, they need a strong background in pathology, which is clearly impractical. Therefore, AI may be the best choice to aid in endoscopic diagnosis. Kumagai et al. have shown that the performance of the system using higher magnification images is better than the system using lower magnification images. However, there was no stratification analysis of superficial and advanced esophageal cancer in this study. The results may not accurately reflect the ability of endoscopy combined with AI to diagnose early esophageal cancer. High-resolution microscopy (HRME) can be used to observe esophageal mucosal tissue and cell morphology. Shin et al tested the ability of different imaging features to distinguish tumors from non-tumor lesions, and the best features were selected with 84% sensitivity and 95% specificity. .
3. The role of AI in histopathological diagnosis of early esophageal cancer
Although AI combined with endoscopic diagnosis has made much progress, endoscopic diagnosis still cannot replace the gold standard in pathology. However, there is a problem in the pathological diagnosis of early esophageal neoplasia; that is, the accuracy of dysplasia diagnosis is not ideal with significant variation between the host of observations. To address this issue, Sabo et al established 2 models to distinguish non-dysplasia (ND) from low-grade dysplasia (LGD) and LGD from high-grade dysplasia (HGD) by image extraction. pathological section stained with hematoxylin and eosin (HE), characteristics of patients with Barrett's esophagus BE. The results showed that the two models performed well in the diagnosis of indistinguishable contour lesions. Baak et al combined the HE-stained cross-sectional imaging features with the immunohistochemical indices p53/Ki67 and used endoscopic gastrointestinal resection specimens and biopsies. Barrett's esophagus for testing. It was found that the system performed well in distinguishing ND from LGD and LGD from HGD; however, the accuracy of distinguishing HGD from intramucosal carcinoma needs to be improved. The performance of the system is better than that of a general pathologist and only slightly worse than that of an experienced pathologist.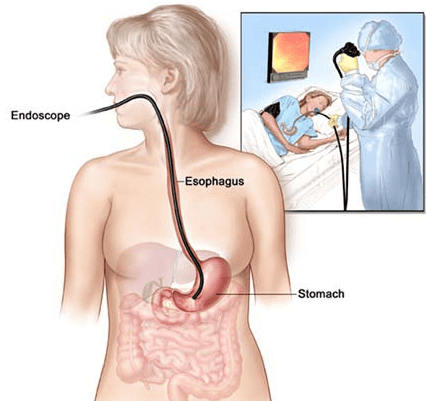
Mặc dù AI kết hợp chẩn đoán nội soi đã có nhiều tiến bộ nhưng chẩn đoán nội soi vẫn không thể thay thế tiêu chuẩn vàng trong chẩn đoán bệnh lý
4. The role of AI in genetic diagnosis of early esophageal cancer
As mentioned above, the invasiveness of endoscopic diagnosis and the variability of pathological diagnosis, together with recent advances in the pathogenesis of esophageal cancer and the development of omics technologies different, made early EC gene diagnosis a hot research topic. Zhang et al and Yu et al used microRNAs and long noncoding RNAs specifically expressed in patients with esophageal squamous cell carcinoma to establish diagnostic models, and the results showed that both Both can be used to effectively differentiate early from advanced tumours.5. The role of AI in risk stratification of early esophageal cancer
It is estimated that only 0.12%-0.43% of patients with Barrett's esophagus may progress to early esophageal cancer each year, making it particularly important to establish an effective model for predicting risk. early esophageal cancer each year in patients with Barrett's esophagus. Previously risk stratification was based primarily on the presence of dysplasia, but its efficacy was not ideal. Critchley-Thorne et al established a predictive model based on characteristic differences in immunofluorescence markers and histopathology between Barrett's esophagus patients who developed early esophageal cancer. per year and those who do not have the disease. Results have not been encouraging, with more than 30% of Barrett's esophagus patients developing early esophageal cancer each year classified as low-risk. Li et al established a prediction model based on single nucleotide polymorphism differences in the biopsy tissues of Barrett's esophagus patients with good performance to predict early esophageal cancer each year.
Người ta đánh giá rằng chỉ 0,12% -0,43% bệnh nhân Barrett thực quản có thể tiến triển thành ung thư thực quản sớm mỗi năm
6. Conclusion
Artificial intelligence AI is trying to be used for endoscopic detection, pathological diagnosis, genetic diagnosis, and early esophageal cancer risk prediction. It is useful for endoscopists and pathologists to improve diagnostic accuracy and assist physicians in treatment and follow-up strategies.Currently, screening for gastrointestinal cancer is a scientific and effective measure for early detection of gastrointestinal cancer (esophageal cancer, stomach cancer, colon cancer) and giving a treatment plan. best treatment. Currently, Vinmec International General Hospital has a package of screening and early detection of cancers of the gastrointestinal tract (esophagus - stomach - colon) combined with clinical and paraclinical examination to bring the most accurate results. maybe.
When screening for gastrointestinal cancer at Vinmec, you will receive:
Gastrointestinal specialty examination with an oncologist (by appointment). Gastroscopy and colonoscopy with an NBI endoscope with anesthesia. Peripheral blood count (laser counter). Automated prothrombin time test. Automated thrombin time test. Activated Partial Thromboplastin Time (APTT) test using an automated machine. General abdominal ultrasound
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
References:Bray F , Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018; 68 :394-424. [PubMed] [DOI] Hur C, Miller M, Kong CY, Dowling EC, Nattinger KJ, Dunn M, Feuer EJ. Trends in esophageal adenocarcinoma incidence and mortality. Cancer. two thousand and thirteen; 119 :1149-1158. [PubMed] [DOI] Thrift AP . The epidemic of oesophageal carcinoma: Where are we now? Cancer Epidemiol. 2016; 41 :88-95. [PubMed] [DOI] Lu-Ming Huang, Wen-Juan Yang, Zhi-Yin Huang, Cheng-Wei Tang, Jing Li, Artificial intelligence technique in detection of early esophageal cancer, World J Gastroenterol. Oct 21, 2020; 26(39): 5959-5969