This is an automatically translated article.
Urinary TB or urogenital TB is a fairly common form of extrapulmonary TB. Cases of patients with repeated diagnoses of urinary tract infections need to be differentiated from UTIs, especially in subjects at high risk for TB infection. Therefore, the appointment of diagnostic tests for urinary tuberculosis in these cases is very necessary.
1. What is urinary tuberculosis?
Urinary TB or urogenital TB is defined as an infection caused by Mycobacterium tuberculosis in the urinary tract and/or genital organs. The route of infection to these organs is usually hematogenous transmission from the foci of chronic lung infection to the kidneys, ureters, bladder and testes, prostate gland in men or ovaries, and fallopian tubes in women. .
Particularly in the urinary system, tuberculosis in the kidney usually starts first with many granulomatous tumors such as metastases, destruction of renal parenchyma, fibrosis or the formation of chronic abscesses. The bacteria then spread to the pelvis, affecting the ureters, bladder, and urethra.
Tuberculosis of the ureter often causes narrowing of the ureters and sometimes causes fluid retention in the kidneys. Bladder tuberculosis is also secondary to renal TB and usually begins at the ureteral orifice, presenting initially as superficial inflammation with edema, granulation, and later fibrosis. However, for urethral TB, this is secondary to genital TB. Patients with genital and urethral tuberculosis often have tuberculous ulcers on the surface of the genital tract.
However, no matter which part is affected in urinary tuberculosis, clinical symptoms are difficult to distinguish the location as well as distinguish it from common bacterial urinary tract infections. At that time, the patient was diagnosed with repeated UTIs but had a very poor response to antibiotics. Therefore, the appointment of diagnostic tests for urinary tuberculosis in these cases is very necessary.
The diagnostic tests for urinary tuberculosis that need to be done will be continued in the following sections.
Lao tiết niệu do nhiễm trùng Mycobacterium tuberculosis gây ra
2. PPD skin test for TB diagnosis
Intradermal injection of purified tuberculin protein derivative (PPD) is an important way of detecting latent tuberculosis. Post-injection skin that is painful, red, and edematous with a diameter greater than 10mm will be considered a positive result, and a diameter greater than 15mm may become evidence of active tuberculosis.
However, tuberculin skin test results can be positive in up to 90% of patients, especially in areas where TB is endemic. Furthermore, if the test is falsely negative, the possibility that the patient has a malignancy, immunosuppressive state, liver disease, and malnutrition should be excluded. Even so, skin testing is a simple test that is easy to perform in suspected cases of repeated UTIs but does not rule out TB in patients with no prior TB diagnosis. .
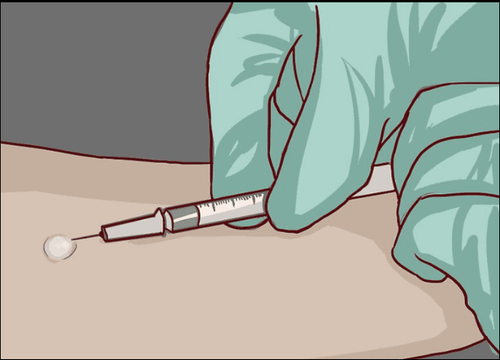
Xét nghiệm da PPD giúp phát hiện bệnh lao thể tiềm ẩn
3. Urine test for TB germs
Early morning urine culture as the first urine sample of the day, at least three with three consecutive mornings, for acid-fast bacilli (AFB) has long been considered the criterion for the diagnosis of tuberculosis urology. This test has a sensitivity of 65% and a specificity of 100%.
Also, urine culture prior to initiation of anti-tuberculosis therapy and sensitivity adjustment in case of resistance is always recommended. The methods of urine culture are quite diverse with many types of media, the time to return results can be after 2-3 days or sometimes more than 4 weeks.
In addition, the AFB test in semen has the same diagnostic value as the urinalysis. However, the risk of foreign contamination to the patient sample is very large, easy to falsify the results, so it is necessary to process the samples immediately after collection.
In addition, the findings of microscopic hematuria and albuminuria on urinalysis will raise suspicion for urinary tuberculosis but do not confirm the diagnosis by urine culture for TB bacilli.

Xét nghiệm nước tiểu tìm vi trùng lao
4. Nucleic acid amplification tests (NAAT)
Nucleic acid amplification tests (NAAT) in patient samples such as urine, semen can give results between 2 and 48 hours. These tests are classified by mechanism as polymerase chain reaction (PCR) assay, ligase chain reaction (LCR) test or PCR variants such as Xpert MTB/RIF.
Among them, PCR test is a widely studied method and has been shown to be very sensitive, specific and rapid to find the presence of bacilli. PCR results are available in about 6 hours.
However, recently, the Xpert MTB/RIF test is gradually replacing, which can simultaneously detect Mycobacterium pathogens and rifampin resistance (RIF) in less than 2 hours. Therefore, this is the initial diagnostic test recommended by the World Health Organization for all patients with signs and symptoms of tuberculosis in general, and urinary tuberculosis in particular.
5. Photographic tools
5.1 X-ray
Chest radiographs may show old or co-existing active TB lesions in patients with urological TB. However, in 50% of patients, chest x-ray results may be negative.
X-rays of the kidneys, ureters, and bladder show calcifications in the kidneys and ureters in about 50% of patients. This can be considered a useful tool to look for evidence of renal or ureteral tuberculosis with calcified nodules.
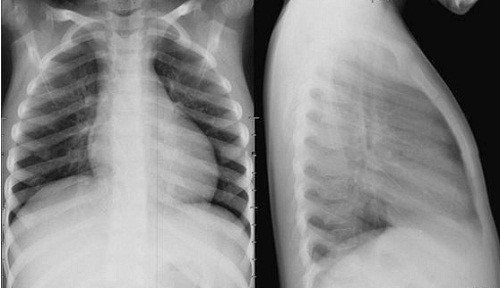
X-quang phổi cho phép chẩn đoán hình ảnh về lao phổi
5.2 Ultrasound
Ultrasound may show cystic lesions, scarring, fibrosis, or chronic abscesses in the kidney due to tuberculosis. Ultrasound is also very sensitive in detecting testicular tuberculosis.
In the case of associated female genital tuberculosis, ultrasound also helps to visualize adhesions in the peritoneum or free fluid in the pelvic cavity. For urogenital TB in men, evidence on sonography is abnormalities, dilation or fibrosis of the epididymis, atrophy, thickening, or calcification of the seminal vesicles, ejaculatory ducts, or prostatitis.
5.3 Computed tomography and magnetic resonance imaging
This imaging tool will become very useful in late or advanced stage to assess the extent of disease and indirect functional status of affected kidney compared with normal contralateral kidney. At the same time, computed tomography and magnetic resonance imaging are also very sensitive to detect signs of calcification in the parenchyma and wall thickness of the ureter and bladder.

Chụp cộng hưởng từ cho hình ảnh chẩn đoán chính xác cao
5.4 Retrograde urography
Retrograde urography is an imaging tool for urological tuberculosis with a sensitivity of 88-95%. This test also helps determine the extent and severity of the disease.
The earliest changes that can be detected by retrograde urography are lesions in the renal parenchyma. In addition, the findings of foreskin and ureteral stenosis would be early suggestive of urinary tuberculosis. As the disease progresses, the later findings are renal parenchymal necrosis, calcified nodules and lesions associated with scarring and narrowing at the ureter and bladder.
5.5 Tissue biopsies
Consider biopsies of genital sores that can help diagnose TB as a cause.
For local lesions in the bladder, especially if scattered from the ureteral orifice, biopsy results not only help to identify TB but also help differentiate from malignancy. In addition, fine-needle aspiration is also a minimally invasive technique that plays a major role in the definitive diagnosis of epididymitis. The probability that acid-resistant bacilli (AFB) can be detected on a smear with this specimen is 60%.
The histological findings of tuberculous ulcerative lesions of the urinary system are similar to those of tuberculosis elsewhere in the body. It is the presence of mycobacteria and the formation of granulomas with nonspecific inflammatory infiltrates, eventually leading to fibrosis and calcification of varying degrees.

Sinh thiết mô giúp chẩn đoán nguyên nhân gây bệnh là do lao.
5.6 Other tests
In addition to the diagnostic tests for urinary tuberculosis as mentioned above, a number of other tests may be necessary in assessing the patient's general condition as well as the ability to respond to treatment.
Specifically, peripheral blood cell count, erythrocyte sedimentation rate, and C-reactive protein quantification are useful for assessing disease severity, renal function, and favorable prognosis for response. with anti-tuberculosis drugs. Erythrocyte sedimentation rate is often increased in patients with epididymal TB in particular and urinary tuberculosis in general; At the same time, when values return to normal can help assess adherence to treatment.
In addition, testing for the presence of human immunodeficiency virus (HIV) should be performed for all patients with TB, not just urinary TB.
In summary, urinary tuberculosis is a diagnosis that should be actively considered in patients with a history of repeated urinary tract infections and especially those at high risk of infection. At this time, the selection and appointment of the appropriate diagnostic test for urinary tuberculosis will help in the correct diagnosis and effective treatment for the patient.
For detailed advice, please come directly to Vinmec health system or register online HERE.













