This is an automatically translated article.
Posted by Master, Doctor Mai Vien Phuong - Gastrointestinal Endoscopy - Department of Medical Examination & Internal Medicine - Vinmec Central Park International General Hospital
Helicobacter pylori is the main cause of stomach ulcers and many other diseases. Currently, there are many methods to treat H. Accordingly, antacids prescribed to treat this disease have also yielded many good results.
1. Helicobacter Pylori bacteria cause many gastrointestinal diseases
Helicobacter pylori (H. pylori) is a spiral with flagellate, gram-negative, aerobic bacteria that inhabit the human gastric mucosa and the course of infection can last for decades. H. pylori infection is thought to be the most common bacterial infection, and affects approximately 50%-75% of the population worldwide. H. pylori is a major cause of upper gastrointestinal diseases, including peptic ulcer disease (stomach and duodenum), chronic gastritis, gastric cancer, and mucosal connective tissue lymphoma. stomach.
Along with upper gastrointestinal problems, H. pylori causes chronic inflammation and low levels in the stomach lining, which can lead to a number of metabolic disorders. H. pylori infection may be correlated with insulin resistance, increased total and low-density lipoprotein cholesterol, and decreased high-density lipoprotein cholesterol in infected individuals. In addition, H. pylori has an important role in other extra-gastric diseases such as chronic urticaria.
The treatment of H. pylori remains a challenge, as there are many factors that determine the success of therapy such as primary or secondary antibiotic resistance, mucosal drug concentrations, patient compliance , side effects and costs. While no new drugs have been developed, current therapy is still based on different mixtures of known antibiotics and antacids.
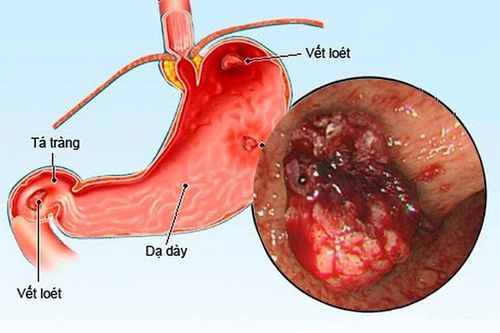
Vi khuẩn H.Pylori là nguyên nhân chính gây viêm loét dạ dày
2. Some current treatment regimens for H.Pylori
A standard triple therapy consisting of two antibiotics and a proton pump inhibitor is suggested as first-line therapy. Bisthmuth-containing quadruple therapy, sequential or quadruple bisthmuth-free therapy (concurrently) is also an alternative therapy. Levofloxacin containing a regimen I of a triple drug is recommended as a life-saving treatment for H. pylori infection after failure of first-line therapy. Antibiotic resistance rapidly reduces the effectiveness of any regimen associated with these remedies. Therefore, the addition of probiotics to the drug, the development of anti-H.Pylori drugs by photodynamic therapies, and the successful achievement of an H. pylori vaccine may hold promise for synergistic or synergistic results against H. pylori, because each has different effects.
2.1. Treatment of H.Pylori in patients allergic to Penicillin
In penicillin-allergic patients, for first-line therapy, bismuth quadruple therapy appears to be a better choice than the PPI-clarithromycin-metronidazole combination regimen. As a lifesaving regimen, a regimen containing levofloxacin plus clarithromycin and a PPI is a second-line treatment in the presence of penicillin allergy.
The Maastricht IV/Florence consensus report recommended the use of antibiotic susceptibility testing (culture-guided therapy), after failure of second-line therapy. However, culture-guided third-line therapy has been recommended, but if antibiotic sensitivity data are not available, empiric triple or quadruple therapy may be recommended as regimen. third line.
Therefore, during the last 30 years when H. pylori was identified, many treatment regimens were proposed, but a single treatment regimen was most effective and least harmful for treating H. pylori infection in patients. all instances are reported as still missing.

Bệnh nhân mắc H.Pylori nhưng lại dị ứng với Penicillin sẽ áp dụng liệu pháp điều trị bộ 4 thuốc chứa bismuth
2.2. Anti-acids PPI
Treatment of H. pylori involves a combination of antibacterial agents (antibiotics) and anti-acids (PPIs) for 7 to 14 days. PPIs inhibit parietal cells H + / K + adenosine triphosphatase (ATPase), the enzyme of the tubular membrane of gastric parietal cells responsible for the final step in gastric acid secretion. Inhibition of this enzyme is more effective than H2-receptor antagonists in inhibiting gastric acid secretion.
At low pH, PPIs in the stomach as an acid-activated prodrug convert to the spiro-intermediate of dihydrobenzimidazole, which then undergo aromaticization to sulfenic acid, which is finally dehydrated to form a quaternary sulfonamide ring. PPIs bind to various cysteines in the α subunit of H+/K+ ATPase and inhibit the enzyme.
PPIs with anti-secretory effects reduce acid production from the stomach, allowing tissues damaged by infection to heal. PPIs can also make acid-labile antibiotics more stable when gastric pH is increased and can also alter antibiotic concentrations by transporting antibiotics from plasma into gastric juice and increasing the rate of successful eradication.

Thuốc kháng tiết axit PPI giúp điều trị H. pylori
3. The role of anti-acid drugs
Several studies have provided conflicting data on H. pylori eradication rates among CYP2C19 genotypes using PPI-based regimens. Several examples of the relative effects of the CYP2C19 pathway on PPI metabolism have been demonstrated. Lansoprazole or omeprazole-based triple therapy was affected by CYP2C19 genotype status, whereas esomeprazole or rabeprazole-based triple therapy was not [30,33,34]. Dosage and duration of PPI therapy in adults correspond to those that inhibit gastric acid secretion. Long-term omeprazole therapy in H. pylori-positive patients induces changes in mucosal inflammation and gland atrophy. PPI-induced hyperglycemia and atrophic gastritis in patients with H. pylori infection may promote the development of gastric cancer.
Zole plus amoxicillin and metronidazole. The cure rate of patients was 82.4% according to ITT analysis and 88.2% according to PP analysis. Based on several existing clinical trials, it seems likely that quinolone-based triple therapy would be effective as first-line therapy in H. pylori infection. The use of levofloxacin as an alternative to clarithromycin in triple therapy and sequential therapy was studied by Qian et al. 7-d triple therapy of levofloxacin (levofloxacin, amoxicillin, esomeprazole) produced no therapeutic effect. satisfactory results, only sequential therapy containing levofloxacin achieved a satisfactory outcome.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
References
1. Lv ZF, Wang FC, Zheng HL, Wang B, Xie Y, Zhou XJ, Lv NH. Meta-analysis: is combination of tetracycline and amoxicillin suitable for Helicobacter pylori infection? World J Gastroenterol . 2015;21:2522-2533. [PubMed] [DOI]
2. Hajimahmoodi M, Shams-Ardakani M, Saniee P, Siavoshi F, Mehrabani M, Hosseinzadeh H, Foroumadi P, Safavi M, Khanavi M, Akbarzadeh T. In vitro antibacterial activity of some Iranian medicinal plant extracts against Helicobacter pylori. Nat Prod Res . 2011;25:1059-1066. [PubMed] [DOI]
3. Buzás GM. Metabolic consequences of Helicobacter pylori infection and eradication. World J Gastroenterol . 2014;20:5226-5234. [PubMed] [DOI]
4. Gu H, Li L, Gu M, Zhang G. Association between Helicobacter pylori Infection and Chronic Urticaria: A Meta-Analysis. Gastroenterol Res Pract . 2015;2015:486974. [PubMed] [DOI]
5. Ben Chaabane N, Al-Adhba HS. Ciprofloxacin-containing versus clarithromycin-containing sequential therapy for Helicobacter pylori eradication: A randomized trial. Indian J Gastroenterol . 2015;34:68-72. [PubMed]
6. Olokoba AB, Obateru OA, Bojuwoye MO. Helicobacter pylori eradication therapy: A review of current trends. Niger Med J . 2013;54:1-4. [PubMed] [DOI]
7. Maliheh Safavi, et al., Treatment of Helicobacter pylori infection: Current and future insights. World J Clin Cases. Jan 16, 2016; 4(1): 5-19