This is an automatically translated article.
Noninvasive ventilation has been shown to be effective in the treatment of acute respiratory failure, especially in patients with chronic obstructive pulmonary disease. Non-invasive breathing equipment needs to be prepared 24/24 every day at the hospital to be ready for treatment.
1. Definition of respiratory failure
Respiratory failure is an impairment in the ability to maintain adequate gas exchange, characterized by abnormalities of arterial blood gas pressures. Includes 2 types as follows:
SHH Type 1: PaO2 < 8kPa, PaCo2 has low or normal value. SHH Type 2: PaO2 < 8kPa, PaCO2 > 6 kPa. Respiratory failure can be acute, chronic, or acute on a chronic basis. A clear distinction should be made in order to have the most appropriate treatment regimen, especially in patients with type 2 respiratory failure.
Acute CO2 elevation acute respiratory failure: There is little or no evidence of respiratory disease from Previously, arterial blood gas pressure showed: Normal bicarbonate, low pH, high PaCO2. Acute hypercapnia respiratory failure on chronic background: Patients with pre-existing hypercapnic respiratory failure have acute deterioration, high bicarbonate indices, low pH, high PaCO2. Chronic hypercapnic respiratory failure: There is evidence of chronic respiration, values: high bicarbonate, normal pH, high PaCO2.
2. Arterial blood gas pressure
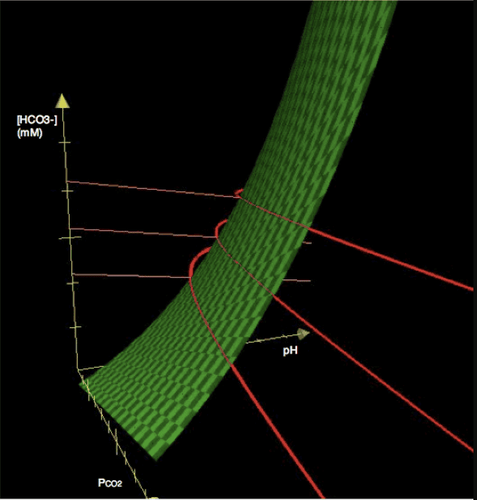
Hình ảnh khí máu động mạch.
Before deciding for a patient to use noninvasive ventilation (NIV), knowledge of arterial blood gases is required. The first step should be to determine the appropriate oxygen therapy regimen and interpret the arterial blood gases based on an understanding of FiO2. There are times when it is necessary to re-measure arterial blood gases to check if the patient needs NIV again.
In addition, arterial blood gas measurement should be considered in all patients with dyspnea severe enough to require hospitalization. In patients with acute respiratory failure with hypercapnia who receive optimal medical care and appropriate oxygen supplementation, arterial air pressure will improve rapidly.
3. Some general introduction to non-invasive ventilators
NIV is not to be used to replace invasive ventilation and endotracheal intubation. The effectiveness of the NIV method has been largely demonstrated in patients with respiratory acidosis (H+ > 45 mmol/L, pH < 7.35). Various NIV ventilators have successfully treated many cases of hypercapnic respiratory failure. If conditions are appropriate, the same type should be used in each clinical area to facilitate training in use. Select the size of face mask, nose mask, nose pad for NIV in the interface. Both facial and nasal markings have been used successfully for patients with respiratory failure with increased CO2 in acute cases, facial marks should be used from the beginning and replaced after 24 hours of implementation.
4. Indications and contraindications of the method.

Tràn khí màng phổi nên dẫn lưu ở liên sườn trước khi tiến hành điều trị
4.1 Indication of NIV is applicable as a therapeutic trial. If NIV fails, endotracheal intubation is performed. Consider in patients with acute COPD (chronic obstructive pulmonary disease) whose respiratory acidosis (H+ > 45 mmol/L, pH < 7.35) persists despite intensive medical care and treatment. Continuous positive airway pressure (CPAP) has been shown to be effective in patients with acute cardiac pulmonary edema, whose tissue oxygenation remains reduced despite aggressive medical therapy. Indicated for patients with acute exacerbation of hypercapnia respiratory failure due to neuromuscular disease or chest wall malformation. Both NIV and CPAP are successful in cases of sleep apnea or decompensated obstruction. Observation of the risk of pneumothorax in epithoracic patients receiving NIV or CPAP should be monitored in the ICU. NIV is used when successful invasive weaning is successful and should be used when conventional weaning fails. In addition, NIV is also used in acute respiratory distress syndrome, respiratory failure after surgery or transplant,... 4.2 Contraindication NIV is not used for patients after respiratory surgery or surgery. Recent facial surgery, there are manifestations of burns, trauma, airway obstruction,... NIV is contraindicated in cases of upper respiratory tract surgery, inability to protect the airways , severe hypoxia, life-threatening, intestinal obstruction, confusion. Use only when endotracheal planning is performed or when implementation leads to noninvasive ventilation. Patients with pneumothorax should have intercostal drainage prior to initiating therapy. After conducting non-invasive ventilatory therapy, clinical assessment, arterial blood analysis, and measurement of oxygen saturation must be performed continuously for 24 hours from the time of implementation. Non-invasive mechanical ventilation should be performed by a respiratory specialist and experienced in handling mechanical manipulations to achieve high safety and effectiveness.
Non-invasive mechanical ventilation is performed at Vinmec International General Hospital with a highly configured ventilator system for ICUs for adults, children and infants.
In particular, the team of doctors performing the technique are all doctors from the Emergency Department with high professional experience.
To register for examination and treatment at Vinmec International General Hospital, please book an appointment on the website for service.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.













