This is an automatically translated article.
Post by Master, Doctor Mai Vien Phuong - Department of Examination & Internal Medicine - Vinmec Central Park International General Hospital
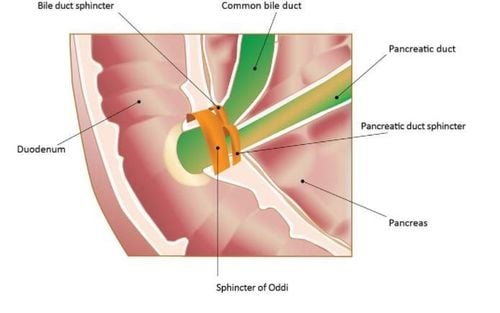
The etiology of the sphincter of Oddi disorder is usually local scarring of the lesion secondary to gallstone removal or surgical manipulation or inflammatory infiltration from a nearby duodenal ulcer or acute pancreatitis. on the papilla. The presence or absence of primary biliary papillary stenosis is controversial, although the finding of a history such as inflammation of the gland is probably the etiology.
Primary or secondary biliary papillary stenosis cannot be clearly distinguished because the presence of gallstones can be considered as a secondary cause, thus factor and the presence of gallstone disease with a single stone Pure papillary traversal can never be ruled out.
1. What is laparoscopic sphincterotomy of Oddi?
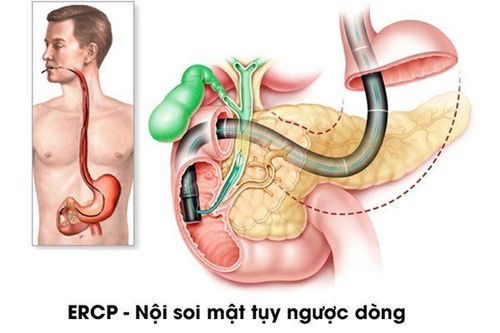
This is a technique to cut part of the sphincter of Oddi to treat the diseases here. Endoscopic Sphinclerotomy (ES) is technically different from surgical sphincleroplasty. In sphincterotomy, the extension line at the top of the great duodenal papilla can be 3 cm long, while endoscopic sphincterotomy does not exceed 1.5-2 cm, so in endoscopic open resection The sphincter must also comply not to exceed this indication. Therefore, the author often uses the word slit or cut open sphincter to understand that this technique is "cutting" more gently than "forming." However, it is necessary to master the technique - if it causes complications that often lead to death - this This is a delicate and sensitive issue that surgeons shy away from when entrusting this task to gastroenterologists to perform sphincterotomy.
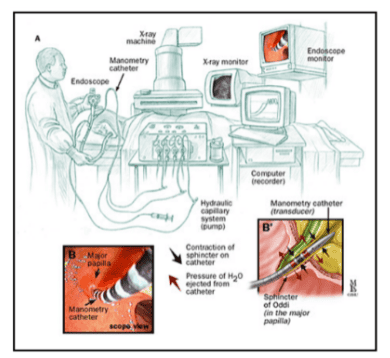
Thủ thuật nội soi mật tụy ngược dòng
2. Taking medicine to treat sphincter disorders
Non-surgical methods (diet and anticholinergics) are not very effective in treating post-cholecystectomy syndrome or sphincter of Oddi disease. Nitrates have sometimes been shown to be effective on the sphincter of Oddi (Butsch, McGowan and Walters 1936) and suggest some prospect of improved treatment (Bar-Meir, Halpern and Bardan 1983).3. Surgical treatment of sphincter disorders
The results reported for detailed sphincterotomy of Oddi with a wide range of variability are generally effective (Gregg 1977, Moody 1977, Raskin 1978, Madura 1981) although not desirable in all cases.
In the Moody, Becker and Potts 1983 report, out of 92 patients with sphincteric sphincter of Oddi-related pain, surgery reduced pain only 43% and with 24% of patients finding no pain relief at all. .
4. Endoscopic sphincter of Oddi for treatment of sphincter disorders
Author Tanaka 1985 performed endoscopic sphincterotomy for 12 patients with duodenal papillary fibrosis who had pain and increased bile duct pressure due to Morphine e response, resulting in complete analgesia in 8 patients. , significantly reduced symptoms in 3 patients and 1 patient with mild pain.
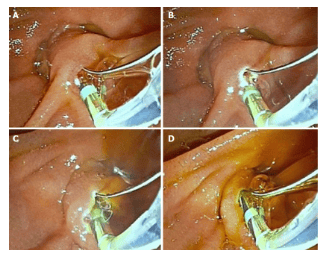
Thủ thuật cắt cơ vòng qua nội soi mật tụy ngược dòng
Morphine-stimulated intrahepatic pressure measurement with morphine was repeated 1-2 weeks after laparoscopic cholecystectomy, no increase in pressure was found in 3 patients although there was a slight increase in pressure in all patients. In another, 2 patients had transient mild pain, the median follow-up was 23 months (5-20 months) during which time had recurrent mild pain in a patient who had already received complete analgesia and One patient had previously experienced pain relief only a few days after laparoscopic cholecystectomy.
5. Efficacy of laparoscopic sphincter of Oddi in relieving pain after cholecystectomy
Further data from the Geenen study on the efficacy of laparoscopic sphincterotomy in relieving pain after cholecystectomy have been recently reported. Forty-seven patients were randomized to undergo endoscopic sphincterotomy or sham procedure. After 1 year of endoscopic sphincterotomy performed in 12 symptomatic patients from a cohort of 24 randomized to sham procedure, sphincter pressure was found to be elevated in 7 patients and normal in 5. patients in this group.
In the 40 patients surveyed and evaluated after 4 years of follow-up and finally 17/18 patients (96%) had sphincter of Oddi dysfunction identified by manometry that was performed by opening the sphincter of Oddi through endoscopically, in patients with normal sphincter of Oddi pressure, endoscopic expansion does not provide significant analgesia relative to the effect of sham procedures, however in most patients with sphincter pressure Normal Oddi (5 ring openers, 2 sham openers) was lost to follow-up after 4 years, even after all patients who lost follow-up responded to sphincter of Oddi, only 59% in the high-pressure group The normal sphincter of Oddi will improve from the enlargement of the sphincter of Oddi.
Roberts-Thomson reported endoscopic sphincter of Oddi opening. In over 300 patients, in 15% of patients with sphincter of Oddi disorder, opening the sphincter of Oddi reduced symptoms in only 51% of patients in this group. With 4 patients with Morphine-Neostigmine test results (Roberts-Thomson and Touli 1985) tested for the second time 6-18 months after laparoscopy. Serum enzyme levels were maintained within the normal range in 2 patients. Two patients had pain unrelated to the second test, whereas two others had pain less severe than the pain due to the Morphine-Neostigmine response prior to sphincter opening.
6. What do other studies say?
In the cholangiography study Shaffer et al. 1986 showed that the time required to reach maximal radioactivity in the biliary system was significantly superior in 9 patients with suspected papillary stenosis compared with 35 patients without. symptoms after cholecystectomy. Sphincterotomy (8 endoscopically, one surgically) markedly reduced the time of peak activity in the bile duct as well as an increase in the amount of radiotracer excreted after 45 min. There was also an increase, but not clear, pain relief in 8 out of 9 patients after sphincterotomy Absorption of radiotracer was normal prior to sphincterotomy in one patient with persistent pain following sphincterotomy. The biliary tract demonstrated decreased absorption and emptying in one patient with recurrent symptoms after a period of analgesia following sphincterotomy Complications with endoscopic sphincterotomy in 7 Patients (13.7%) were found to have complicated duodenal papillary fibrosis occurring in 3 of 34 patients (8.8%) with bile duct dilatation or delayed drainage, whereas 4 out of 17 patients Patients (23.5%) with normal bile ducts endured a complication of sphincterotomy of Oddi.The difference in complication rates of these two groups of patients was statistically significant. that the complication rate of myostomy Endoscopic loop of Oddi was significantly higher when indicated for duodenal papillary fibrosis compared with stricture due to common bile duct stones, especially when the biliary tract was not dilated.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.