This is an automatically translated article.
Post by Master, Doctor Mai Vien Phuong - Department of Examination & Internal Medicine - Vinmec Central Park International General Hospital
Recently, H. pylori infection or H. pylori gastritis was observed to be associated with iron deficiency anemia (IDA), and eradication therapy was reported to be effective in improving levels ferrintin or even cure iron deficiency anemia. A similar relationship between idiopathic thrombocytopenic purpura (ITP), a common hematological disease in children, and H. pylori infection has also been revealed in a number of clinical studies conducted by physicians.
Ban xuất huyết Henoch-Schonlein ở tá tràng
1. Causes of Henoch-Schonlein purpura
Henoch-Schonlein purpura (HSP) is a common disease in children. It is characterized by IgA deposition in the renal vessel wall and mesoderm and is defined as acute leukocytosis of the small vessels. Although it is known that the causes of Henoch-Schonlein purpura are variable, infectious agents are considered to be the most important etiological factors. In addition to purpura, gastrointestinal manifestations, commonly noted as abdominal pain and bleeding in the gastrointestinal tract, co-occur in the course of the disease and are related to treatment strategy and prognosis. On the other hand, the prevalence of H. pylori infection ranges from 20% to 80%, which makes its infection widespread worldwide. Patients are primarily infected at an early age and remain carriers throughout life. A small number of infected people will develop upper gastrointestinal disorders, the majority of whom are asymptomatic for life. Therefore, many of these children are diagnosed only after other diseases cause intestinal manifestations.
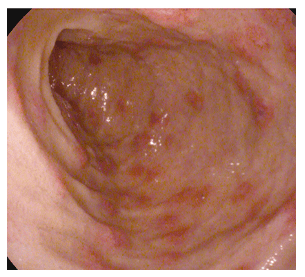
Ban xuất huyết Henoch-Schonlein ở ruột non một bé gái ba tuổi
2. H.Pylori infection and Henoch-Schonlein purpura
A possible association between H. pylori infection and Henoch-Schonlein purpura was first demonstrated by several case reports in adults with Henoch-Schonlein purpura and concurrent gastritis. The H. pylori infection can be detected by all 13 C-urea breath tests. The gold standard of diagnosis is based on gastric mucosal biopsy. Reinauer et al. reported that in a case of Henoch-Schonlein purpura and chronic gastritis with H. pylori with diagnosed infection, the purpura, intestinal symptoms, and albuminuria disappeared after treatment. eradication treatment. However, the patient was found to be reinfected while the purpura recurred 10 months later, while the symptoms improved after H. pylori eradication. Mozrzymas et al., and Mytinger et al., respectively, present cases of children with this problem. It has also been reported that in children with Henoch-Schonlein purpura and duodenal ulcers, purpura manifestations improved following H. pylori eradication.3. What do the studies say?
Different from the literature on cases in Western countries, quite a few studies in some Asian countries have enough sample size to carry out the cohort study, so the results may be more reliable. Yuan et al. reported a retrospective study with the largest sample size, including 186 Henoch-Schonlein purpura patients and 150 controls. The anti-Hp IgG test is used as a diagnostic method to detect H. pylori infection. Forty-nine percent (76/186) of the patients in the Henoch-Schonlein purpura group and 15.3% (23/150) of the controls were confirmed infected. Based on the results, the authors concluded that infection was associated with the occurrence of Henoch-Schonlein purpura. In another study with the largest follow-up sample, Li et al. stated that OCA eradication treatment (O: Omeprazole; C: Clarithromycin; A: Amoxicillin) was effective in preventing recurrence of purpura Henoch-Schonlein in concurrent H. pylori infections confirmed by rapid urease test (RUT). A meta-analysis was performed to obtain the combined prevalence of H. pylori infection and determine the relative relationship between the two diseases. One thousand three hundred and nine cases, including 749 children with Henoch-Schonlein purpura and 560 healthy controls, were included in the cohort analysis. The prevalence of pediatric Henoch-Schonlein purpura shows a wide range, from 22% to 75%, while the prevalence is only 3% to 44% in healthy controls. Using data from 10 studies, the meta-analysis concluded that infection with this bacterium was statistically significantly associated with an increase in Henoch-Schonlein purpura with almost 4 times the risk in children in some Asian countries. This study also stated that eradication therapy may have a protective role in the recurrence of Henoch-Schonlein purpura, based on data from the 4 available studies (RR = 0.38, 95% CI: 0.25-0.58, P < 0.001) The prevalence of Henoch-Schonlein purpura reported in several Asian countries varies by region. Interestingly, the prevalence in children with Henoch-Schonlein purpura Schonlein has been reported in a number of different Asian countries across regions, possibly as a result of a combination of different rates of H. pylori infection and prevalence of Henoch-Schonlein purpura. In addition, the researchers agree that there is geographic variation of different strains of H. pylori around the world. Cytoxin-linked cytotoxin-linked A (Cag-A) gene-positive strains predominate among East Asian H. pylori isolates, while cag-A-negative can be identified in 20% to 40% strains from Europe or Africa. Cag-A-positive H. pylori strains from the above continent show differences in the number of repeats with each other, leading to the infectivity of the variants to the host and to induce manifestations . A similar situation is observed when considering vacA, another important virulence factor for H. pylori. This may be the basis for why cases of Henoch-Schonlein purpura and H. pylori infection are rare in Western countries (especially developed countries) but are common in Eastern regions. ASIAN. Therefore, the current basis for assuming a potential relationship between H. pylori infection and Henoch-Schonlein purpura in Westerners may not be as strong as in Easterners. Gastroduodenal endoscopy in patients with Henoch-Schonlein purpura
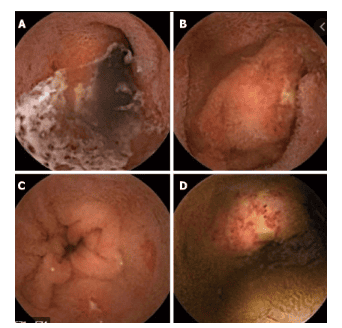
In these patients with obvious abdominal symptoms, endoscopy is considered a useful tool to confirm the diagnosis and rule out other complications. other surgical emergencies. It was reported that the duodenum was the most common site of injury, with other sites such as the stomach, body, and curvature angles, but never the cardia or esophagus. Endoscopic findings including congestion, edema, petechiae, ulcers, and other endothelial lesions include the common endoscopic findings of Henoch-Schonlein purpura. These manifestations more or less overlap with those of H. pylori infection, so detection of the bacteria is important in the treatment of some patients.
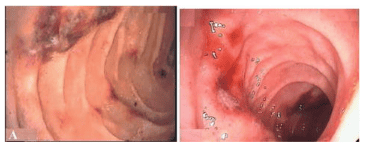
Hình ảnh nội soi ban xuất huyết Henoch-Schonlein ở tá tràng
It is not possible to distinguish the duration of H. pylori infection during the progression of Henoch-Schonlein purpura using current research evidence
Intestinal manifestations can present at any stage. of the Henoch-Schonlein purpura course, which will be the clue to detect H. pylori infection. There is no evidence that can clarify whether the patient was infected before or after the symptoms of Henoch-Schonlein purpura appeared. It has been reported that the level of anti-H. pylori IgG is relatively higher in the serum of Henoch-Schonlein purpura patients, compared with healthy controls, while it is far from revealing the effect of bacterial infection. for this autoimmune disorder. Even clinic studies have shown a strong relationship between H. pylori infection and Henoch-Schonlein purpura; Researchers were unable to confirm that bacterial infection caused the development of Henoch-Schonlein purpura. In addition, although Henoch-Schonlein purpura can be triggered by other infections, namely some respiratory infections, the limitation of their retrospective background makes exclusion impossible. except for all infectious diseases or allergies.
There are still many unanswered questions to be answered
Although several investigations have linked H. pylori infection with Henoch-Schonlein purpura in children, many questions remain unanswered. Answers need to be answered, which may lead to a deeper understanding of the role of H. pylori in Henoch-Schonlein purpura, and to improved treatment and prevention strategies: (1) The clinic's latest report contains significant limitations in terms of sample size and study methods. Large-scale clinic-based prospective studies or nationwide epidemiological studies are needed to confirm a correlation or causal relationship between H. pylori infection and Henoch-Schonlein purpura; (2) Most of the current clinical studies are from Asia, especially from China. Researchers may need to consider whether highly virulent H. pylori strains differ from low virulence strains in causing or exacerbating Henoch-Schonlein purpura; (3) Further studies are also required to find out if H. pylori infection is the cause of Henoch-Schonlein purpura or just a concurrent infection; (4) It is also important to know whether the persistence of H. pylori causes abdominal manifestations during the progression of Henoch-Schonlein purpura; (5) Intensive long-term follow-up is required for recurrent Henoch-Schonlein purpura after radical therapy to determine a possible relationship between Henoch-Schonlein purpura and H. pylori infection, and to see its efficacy. of such treatment in relapse control; (6) Future studies answer whether endoscopy can be an additional diagnostic tool when a patient with Henoch-Schonlein purpura is suspected to have significant gastrointestinal symptoms but no purpura typical or not; and (7) The underlying mechanism of the cross-link between the two diseases requires more research to elucidate.
Conclusion
Extragastric disturbances are important aspects of H. pylori infection and associated disease progression, which has been demonstrated by an increasing number of clinical studies in children. Current studies suggest a potential relationship between infection and Henoch-Schonlein purpura in children. Therefore, detection of H. pylori carrier status in children with Henoch-Schonlein purpura, especially those with abdominal manifestations, is indispensable in endemic areas. Diagnostic methods that can confirm current infection are recommended to detect the presence of H. pylori in patients with Henoch-Schonlein purpura. However, it remains unclear how bacterial infection is involved in the progression of Henoch-Schonlein purpura. Review of the efficacy of eradication therapy in children with Henoch-Schonlein purpura Without H. pylori infection, stronger evidence, such as randomized, placebo-controlled studies, Large, double-blind, with appropriate diagnostic methods, will be conducted to reveal the potential association between H. pylori and Henoch-Schonlein purpura and to assess whether any type of therapy should be instituted. use in these children.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.