Acromioclavicular joint dislocation is one of the most common shoulder injuries. Most of the cases are caused by direct impact on the shoulder. After a fall, the patient will often feel pain and swelling in the shoulder area, along with the outer clavicle protruding, creating a bump above the shoulder.
There are many classifications to assess the degree of acromioclavicular joint injury, but the Rockwood classification is the most used by doctors. According to this classification, the injuries are classified into 6 levels. For types I and II, conservative treatment usually delivers good results. Indications for surgery are usually made for injuries of Type III or higher. For acromioclavicular joint injuries of Type I and II, the patients are treated conservatively by wearing a fixed belt. The patients should be instructed on how to monitor and adhere to immobilization and return for re-examination after 3-6 weeks (since the injury) to assess joint stability and progression of symptoms.
If at 3 months after the shoulder injury, a patient with acromioclavicular joint dislocation still experiences shoulder pain and feels a clicking sound when moving the shoulder, and radiographic examinations show the lateral clavicle protruding much above the apex of the shoulder, the patient will be indicated for chronic acromioclavicular joint dislocation. In such cases, surgical treatment is necessary to improve the instability of the acromioclavicular joint.

There are many surgical methods for chronic acromioclavicular joint dislocation and they can be divided into two main groups, namely open surgery and laparoscopic surgery. Both of these methods require surgical reconstruction of the coracoclavicular ligament to ensure long-term stability of the acromioclavicular joint. Each method has its own advantages and disadvantages and has been gradually developed thanks to the progress in specialized knowledge, tools, and, in particular, the development of supporting equipment for shoulder arthroscopic surgery.
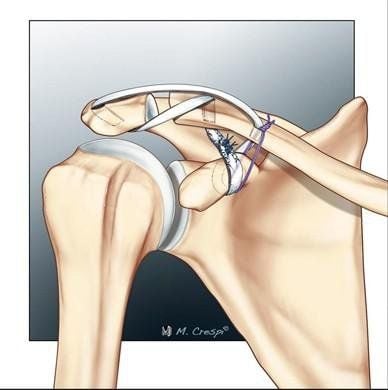
The most classic method for chronic acromioclavicular joint dislocation surgery is Coracoacromial ligament transposition. This technique, described by Weaver and Dunn, surgically removes a portion of the lateral clavicle, then transfers the attachment point of the scapular ligament from the apex of the shoulder to the lateral clavicle to reconstruct the coracoacromial ligament. Later, some authors improved this technique by keeping the position of the clavicle in place with the coracoid process using Hook splints, super-strong surgical thread, TightRope, or tendon grafts to increase stability. This method is relatively effective (70% success rate) in terms of restored functions as well as patient satisfaction. But the disadvantage is that it needs a large surgical area, and requires dissection of many organs, and the use of Hook splints has many complications such as infection and irritation by the splint.
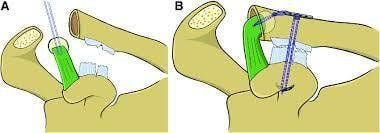
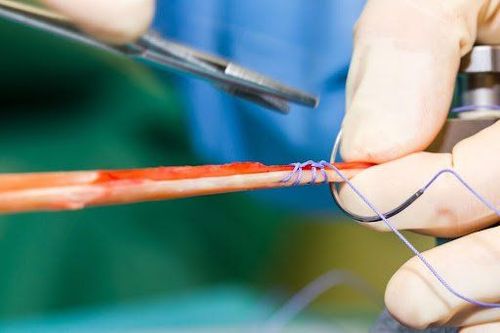
The second method is the technique of using autologous or allogeneic tendons to anatomically reconstruct the broken acromioclavicular and coracoclavicular ligaments. Numerous biomechanical studies have demonstrated the superiority of this technique over traditional methods. In an essence, this method uses tendon grafts (autologous or allogeneic tendons from tendon donors) to create new ligaments, which then be used to reconstruct the acromioclavicular and coracoclavicular ligaments at their original anatomical positions. This helps stabilize the shoulder joint. There are many options when it comes to the selection of autologous or allogeneic tendon grafts, as well as how to create a tunnel to place the tendon and fixate it. With the development of endoscopic techniques, now at Vinmec Times City International Hospital, we are implementing laparoscopic techniques to regenerate ligaments with autologous Hamstring tendons, and fixate the tendons with self-dissolving vis, which have brought good results in terms of postoperative recovery and shoulder functions for patients.
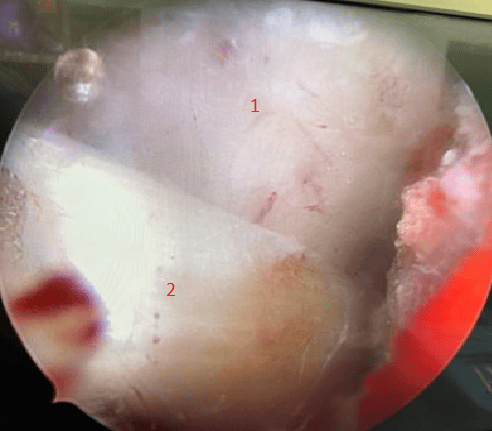
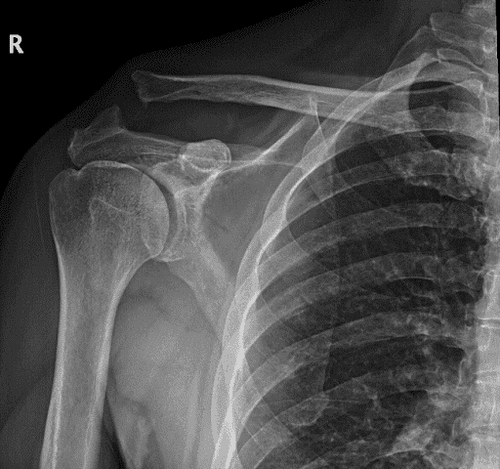
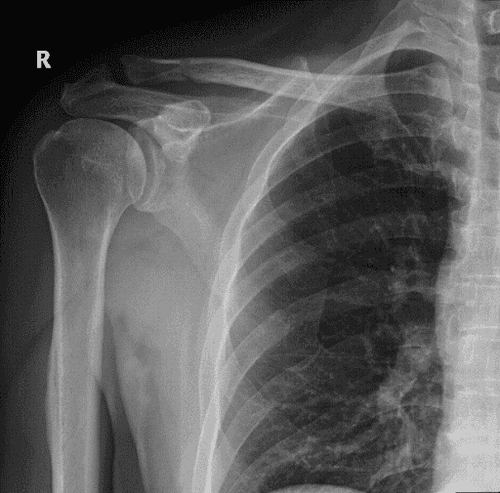
We would like to introduce a case of a 64-year-old male patient. 3 months after falling off a motorbike and hitting his right shoulder directly on the road, after the fall, the patient experienced severe shoulder pain and had to go to the hospital for examination. He was diagnosed with Type III Acromioclavicular Joint Dislocation. He then underwent conservative treatment by wearing Desault's bandage on his right shoulder for 4 weeks. However, 3 months post-injury, the patient still experienced a dull pain in his right shoulder, which got worse when he moved his arm up. It is worth mentioning that the patient loves to play sports and the pain had a great impact on his mental health. After visiting many institutions to no avail, the patient came to us at Vinmec Times City International Hospital. The examination showed that the patient had a lot of pain at the acromioclavicular joint and the outer clavicle was protruding much higher than normal. The X-ray clearly showed that the patient's right acromioclavicular joint was still in dislocation, along with ruptures of acromioclavicular and coracoclavicular ligaments. Realizing that it was a case of chronic shoulder dislocation with a low chance for natural healing of the ligaments, we explained to the patient and opted for shoulder arthroscopic surgery to anatomically reconstruct the patient's acromioclavicular and coracoclavicular ligaments using the patient's own semitendinosus tendon.
After surgery, the patient was stabilized and discharged after 2 days. He had to have his arm immobilized for the next 6 weeks and later started occupational therapy according to the program we set up for the patient. Currently, the patient no longer experiences pain in the acromioclavicular joint and is expected to be able to return to sports - his passion, in 6 months.
Treatment of Type 3 Acromioclavicular Joint Dislocation still remains controversial, especially for elderly patients. For cases of persistent shoulder pain due to chronic shoulder dislocation, surgery is recommended to resolve the pain and help the patient return to a more active life. With many years of experience in shoulder arthroscopic surgery, at Vinmec, we are performing arthroscopic shoulder surgery to anatomically reconstruct the acromioclavicular ligament, and the clavicle using autologous semi-tendon. This is a difficult technique that requires the surgeon to be skilled, highly qualified, and knowledgeable about shoulder arthroscopy. From there, it brings many advantages such as fast recovery after surgery, rebuilding new ligaments like the original, and allowing patients to return to daily activities and sports.
If you are experiencing shoulder, elbow, or wrist problems, please immediately contact MSc, MD Vu Duc Viet (Phone number: 0947860575) of the Department of Upper Limb Surgery - Center for Orthopaedics and Sports Medicine, Vinmec Times City International Hospital or MSc, MD Nguyen Huu Manh (Phone number: 0985202486)
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.













