This is an automatically translated article.
Article written by Master, Doctor Mai Vien Phuong, Head of Gastrointestinal Endoscopy Unit, Department of Medical Examination & Internal Medicine - Vinmec Central Park International General Hospital.
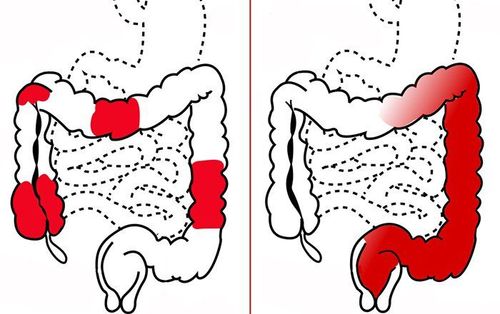
The colon is the large intestine (colon) and the rectum is the last part of the intestine where stool is stored. Ulcerative colitis is a chronic inflammation of the colon and rectum. Small sores can develop on the lining of the colon, bleed, and form pus. In this article, we will learn more about the treatment-resistant or drug-dependent cases of ulcerative colitis
1. Steroid-resistant cases
1.1. Criteria for assessing resistance to intravenous steroids According to ECCO, criteria for assessing resistance to intravenous steroids include a combination of clinical, laboratory, imaging, and endoscopic factors:
Criteria Clinical: If the patient still defecates >12 times/day on the 2nd day of intravenous steroid therapy, the surgical rate is 55%. If the patient has bowel movements > 8 times/day or 3 to 8 bowel movements/day but CRP >45 mg/l on day 3 of intravenous steroid therapy, the surgical rate is 85%. Subclinical criteria: Erythrocyte sedimentation rate > 75mm/hour or temperature on admission > 38°C, the risk of surgery is 5-9 times higher. Imaging/endoscopic criteria: Colon dilatation >5.5 cm, “mucosa island” or bowel obstruction on unprepared abdominal radiographs were all associated with surgical risk in 73-75%. cases. On endoscopy, the severity scale is used as a criterion for assessing response to treatment and switching to other treatment options or surgery. In severe cases, deep ulcers are often found in the lower part of the colon and can therefore be detected by sigmoidoscopy. Total colonoscopy is sometimes difficult to perform in critically ill patients because of the increased risk of perforation. Evaluation of these criteria will help physicians choose whether to switch to other conservative medical treatments, such as cyclosporine, infliximab or tacrolimus, or to undergo early surgery. If medical treatment after 4-7 days does not bring results, it will need to switch to surgery.

Tiêu chuẩn đánh giá kháng trị với steroid đường tĩnh mạch gồm yếu tố lâm sàng, xét nghiệm, chẩn đoán hình ảnh và nội soi.
1.2. Cyclosporin Intravenous Steroid Alternatives The efficacy of Cyclosporin in steroid-failed cases of ulcerative colitis has been demonstrated in clinical trials with treatment response rates ranging from 76 - 85%. The dose of 2mg/kg/day is currently used as the standard dose in initiation of treatment and the rate of surgery at different points in hospital stay, within 3 months, 12 months is 25%, 30% and 30%, respectively. 45%. Time to assess response to treatment is after 4 days.
However, due to narrow indications as well as concerns about side effects, in practice, the proportion of patients treated with cyclosporine is not high. According to a national IBD study in the UK, only 24% of patients with steroid-resistant RA were treated with cyclosporine. For patients treated with cyclosporine who were successfully converted to maintenance oral thiopurine, the incidence of surgery at longitudinal follow-up was significantly reduced. However, in patients who have failed prior thiopurine therapy, cyclosporine should not be selected as salvage therapy.
Tacrolimus This is a calcineurin inhibitor with a mechanism similar to cyclosporine. In a meta-analysis and review study, the clinical response after 2 weeks was significantly higher in the tacrolimus group than in the placebo group. The rate of no surgery at 1 month, 3 months, 6 months and 1 year was 86%, 84%, 78% and 69%, respectively.
Infliximab The use of infliximab (IFX) as a single dose of 5 mg/kg is an effective salvage therapy in severely steroid-resistant patients. A randomized controlled trial reported a significantly lower 3-month surgical rate compared with placebo for patients initially treated with intravenous betamethasone but no response (7/24 vs 14/21, p<0.05). At long-term follow-up, the rate of surgery at 1 year was 35%.
Several studies have investigated the prognostic factors of response to IFX in critically ill patients with/without steroid resistance. At the time of admission, high CRP levels, low albumin, positive pANCA antibodies, and severe endoscopic lesions were associated with a high likelihood of flare-ups or the need for surgery. Complete clinical response at weeks 10-14, endoscopic wound healing, and serum IFX levels above 2.5 μg/ml at week 14 are good prognostic factors for this disease. possibility of no surgery and no recurrence. Low serum IFX concentrations at week 6 or high fecal IFX concentrations during the first days after initiation of treatment predict IFX nonresponse.
Head-to-head studies showed no difference between IFX and calcineurin inhibitors in the treatment of steroid-resistant patients on the criteria of quality of life, surgical rate, mortality, and infection. The choice of salvage therapy depends on the individual patient. Cyclosporine should not be used in patients with low blood cholesterol or 0.1g0e because of the increased risk of adverse effects on the nervous system.
1.3. Cases of resistance to oral steroids For patients with moderate disease activity who are resistant to oral steroids, intravenous steroids or anti-TNF preparations in combination with thiopurine or tacrolimus may be selected.
1.4. Steroid dependence For steroid dependent patients, thieupurine, anti-TNF preparations in combination with thiopurine or methotrexate can be used. In the event of failure, the second regimen may be switched to another biologic, vedolizumab, or surgery may be considered.
The efficacy of anti-TNF agents such as infliximab, adalimumab and golimumab in achieving and maintaining steroid-free remission has been demonstrated in multiple clinical trials with patients receiving initial corticosteroid therapy. The UC-SUCCESS trial demonstrated that the combination of IFX with azathioprine was more effective than IX alone. However, data on the combination of adalimumab or golimumab with immunomodulatory drugs are lacking. When there is no response to an anti-TNF drug, another drug can be switched. A meta-analysis found that treatment response ranged from 23 to 92%, with remission rates ranging from 0 to 50% when switching from IFX to adalimumab.
In the GEMINI trial 1, patients who had received steroid therapy but were dependent on or failed anti-TNF were randomized to receive Vedolizumab or placebo. At week 52, the steroid-free remission rate in the vedolizumab group was 38.5%, which was statistically significantly higher than in the placebo group (13.9%). In addition, no difference was observed in the rates of achieving and maintaining remission between the steroid-dependent and anti-TNF-failure groups.
A multicenter study in patients with steroid-dependent bleeding ulcerative colitis demonstrated a statistically significant higher rate of remission at 16 weeks with methotrexate than in the placebo group. 41.7% versus 23.5%, p<0.05) and better symptom control.

Những bệnh nhân bị phụ thuộc steroid có thể điều trị thieupurine, các chế phẩm anti-TNF phối hợp với thiopurine hoặc methotrexate.
2. Treatment of ulcerative colitis in cases of resistance to immunomodulatory drugs
For patients with advanced bleeding ulcerative colitis who are moderately resistant to thiopurine, anti-TNF can be used in combination with thiopurine. If that fails, another anti-TNF product or vedolizumab can be switched. In case medical treatment does not bring clear clinical effect, surgery should be considered.
Evaluation of resistance to immunomodulatory drugs should be based on endoscopic and histopathological results. It is also important to rule out possible causes of persistent symptoms such as CMV or C.difficile . In the absence of contraindications, anti-TNF agents should be selected. In a Cochrane review, in patients with moderate to severe bleeding ulcerative colitis resistant to steroids and/or immunomodulators, weekly IV IFX was administered at week 0.2. and 6 would have a better rate of clinical symptom complete response week 8 than placebo. Several studies have also shown the efficacy of adalimumab and golimumab in patients who are intolerant to or have failed immunomodulatory therapy. ECCO still recommends that for this group of patients, it is still recommended to combine IX with thiopurine to prevent the creation of antibodies with biological products, as well as to raise the blood concentration of IFX, thereby maintaining the treatment effect. No studies have demonstrated similar pharmacokinetic effects when adalimumab or golimumab are combined with immunomodulators.
Please follow the website: Vinmec.com regularly to update many other useful information.