This is an automatically translated article.
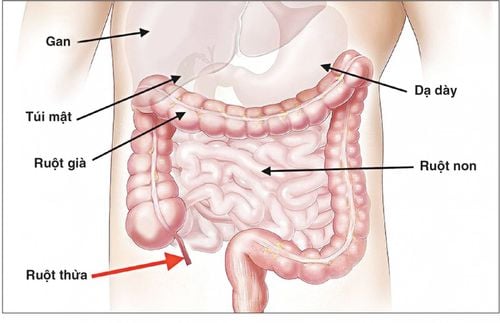
The article is professionally consulted by Master, Doctor Le Hong Chien - Doctor of Radiology - Intervention - Department of Diagnostic Imaging and Nuclear Medicine - Vinmec Times City International General Hospital. The doctor has many years of experience working in the field of diagnostic imaging and interventional radiology (endovascular intervention and extravascular intervention).Digital mesenteric angiography with background erasure is an imaging technique with an iodinated contrast medium to visualize the superior or inferior mesenteric vasculature. These are the arteries that supply blood to the small intestine, colon, and rectum.
1. What is the cause of mesenteric artery occlusion?
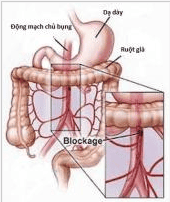
Stenosis of the superior mesenteric artery is one of the most common causes of small bowel ischemia, which can be chronic or acute. There are many causes of vascular stenosis, the most common being atherosclerotic plaque, wall thrombosis, vascular dissection, and fibromuscular dysplasia.The intestinal ischemia has clinical manifestations such as: abdominal cramping pain after each meal and absorption disorders, intestinal mucosa atrophy. In some cases of atherosclerotic plaque, the thrombus that detaches or migrates from the aorta will cause acute embolism, which can lead to intestinal necrosis, which can be life-threatening.

Hẹp tắc động mạch mạc treo tràng trên là một trong những nguyên nhân thường gặp gây thiếu máu ruột non
2. Baseline digitization and dilation, mesenteric artery stenting
In the past, the treatment method for mesenteric artery occlusion was mainly medical treatment combined with surgery to remove thrombus or to bridge the narrow site.Since the 1980s, interventional radiology re-establishes the circulation of the superior mesenteric artery to limit the risk of ischemia and bowel necrosis. Up to now, dilation and stenting of the superior mesenteric artery in combination with medical therapy has become one of the indispensable strategies in the management of patients with acute or chronic ischemic bowel.
2.1 Indications All causes of stenosis of the superior mesenteric artery with symptoms of intestinal ischemia: periodic abdominal pain immediately after eating, CT images (computed tomography) with arterial stenosis, inflammation, intestinal edema due to anemia.
2.2 Contraindications Allergy to Iodine Contrasts Severe renal failure (grade IV) Severe and uncontrolled coagulopathy (prothrombin <60%, INR > 1.5, platelet count < 50 G/l). Pregnant.

Thủ thuật này có chống chỉ định với phụ nữ có thai
3. Procedures for imaging and dilatation, setting the digitized mesenteric artery bracket to erase the background
3.1 Preparations PerformerSpecialist Physician Assistant Radiology Technician Nursing Doctor, anesthesiologist (if patient cannot cooperate) Means
Digital background eraser angiogram (DSA) ) Specialized electric pump Film, film printer, image storage system Lead vest, apron, X-ray shielding Medicine
Local anesthetics General anesthetics (if anesthesia is indicated) Medicines anticoagulant Neutralizing anticoagulants Water-soluble Iodine contrast agents Skin and mucosal antiseptic solutions Common medical supplies
Syringe 1; 3; 5; 10ml Syringe for electric pump Distilled water or physiological saline Gloves, gown, cap, surgical mask Aseptic intervention kit: knife, scissors, tongs, 4 metal bowls, bean tray, tray Cotton, gauze, surgical adhesive tape. Medicine box and first aid kit for contrast drug accidents. Special medical supplies
Angioplasty Needle Insertion Kit 5-6F Standard Lead 0.035inch Angiography Catheter 4-5F Microcatheter 2-3F Micro Lead 0.014-0.018inch Angioplasty Ball Bracket vascular lumen Pressure pump to inflate balloon angioplasty. Guide Catheter 6F Y-connector set. Patient
The patient is thoroughly explained about the procedure to coordinate with the physician. Need to fast, drink before 6 hours. Can drink no more than 50ml of water. In the intervention room: the patient lies on his back, fitted with a monitor to monitor breathing, pulse, blood pressure, electrocardiogram, SpO2. Disinfect the skin, then cover with a sterile, perforated cloth. The patient is too excited, can't lie still: need sedation...

Trước khi thực hiện thủ thuật, bác sĩ sẽ giải kích kỹ càng về thủ thuật với bệnh nhân
Medical record for inpatient treatment There is an approved order to perform the procedure. X-ray, CT, MRI (magnetic resonance) (if any). 3.2 Procedures Diagnostic angiography Local anesthesia, skin incision Femoral puncture (arterial) with 18G needle Insertion of the vascular catheter Intraluminal catheter angiography of the abdomen from the base of the visceral artery with a tail-shaped catheter pig. Selective angiography of the superior mesenteric artery with a Cobra or RH catheter, Yashiro. Approach to the lesion Insert a guide catheter into the root of the superior mesenteric artery Insert the microcatheter and microwire into the superior mesenteric artery through the stenosis to the jejunal and ileal arteries Remove the microwire and replace Replaced with a rigid micro-conductor 0.014- 0.018". Endovascular intervention Insertion of the balloon into a narrow position via a micro-rigid microwire Use a pressure pump to inflate the balloon Withdraw the balloon from the micro-rigid wire Insert the bracket into the narrow position of the artery and open the holder. Postoperative check angiography. Abdominal aorta with pigtail catheter and selective angiography of superior mesenteric artery with Cobra or RH catheter. Finish the trick. 3.3 Evaluation of the results Bracket position: The distal end of the bracket is located at least 5mm below the occlusion site, the proximal end can protrude into the lumen of the aorta but not more than 3mm.
Circulation in and after the rack: the remaining degree of narrowness in the rack frame is not more than 30%. There is no vascular dissection anterior and posterior to the bracket.
3.4 Complications and management Hyperperfusion syndrome: seen in cases of prolonged chronic anemia. After the intervention, the blood flow to the capillaries increased rapidly and suddenly. Clinical manifestations are increased abdominal pain, edematous bowel wall, congestion and possibly ascites (on CT images). These symptoms are likely to subside without intervention. Hematoma in the femoral region (around the common femoral artery puncture site): Bandage compresses the artery opening. Consult an interventional physician to close the bleeding site. Dissection of the superior mesenteric artery wall: Use anticoagulation if ineffective, consult a gastroenterologist. Occlusion of the superior mesenteric artery causing acute intestinal ischemia: Anticoagulation should be used if ineffective, consult a gastroenterologist. Vinmec International General Hospital is a high-quality medical facility in Vietnam with a team of highly qualified medical professionals, well-trained, domestic and foreign, and experienced.
A system of modern and advanced medical equipment, possessing many of the best machines in the world, helping to detect many difficult and dangerous diseases in a short time, supporting the diagnosis and treatment of doctors the most effective. The hospital space is designed in a modern way, but still gives patients the comfort, friendliness and peace of mind as if they were at home.
For detailed information, please contact the hospitals and clinics of Vinmec health system nationwide.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
SEE MOREAre mesenteric tumors dangerous? Small bowel obstruction dangerous? Diagnosis and treatment Diagnosis and treatment of mesenteric lymphadenitis