This is an automatically translated article.
The article is professionally consulted by Specialist Doctor I Tran Thi Ngat - Department of General Surgery - Vinmec International General Hospital Da Nang.Endotracheal anesthesia for endoscopic ventricular septal dissection is an anesthetized method indicated in the case of endoscopic septal defect and ventricular tumour biopsies.
1. Laparoscopy to break through the floor of the ventricles
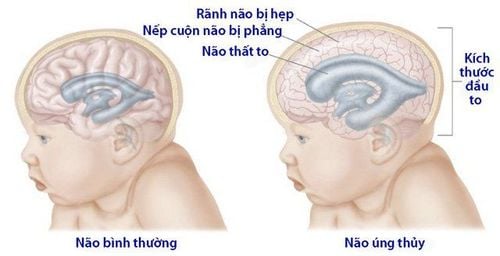
Among brain tumors, pineal gland tumors are rare in children and sensitive to radiation therapy. This tumor blocks the circulation, or other causes cause an imbalance between the absorption and secretion of CSF, causing frequent headaches in children. Over time, the CSF accumulates excessively, causing dilation of the brains. ventricles and increased intracranial pressure.Previously, to solve hydrocephalus, doctors often put a wire (VP Shunt) to guide cerebrospinal fluid down to the peritoneum. However, this technique has some limitations such as: High complication rate, high cost of wire, sometimes blocked tube, tube infection. The endoscopic technique of breaking the floor of the ventricles has limited these defects and helped increase the ability to recover quickly after surgery.
2. What is endotracheal anesthesia?

Gây mê nội khí quản
Endotracheal anesthesia for endoscopic ventricular septal defect is indicated in cases of endoscopic septal defect and ventricular tumour biopsies.
This technique is contraindicated if:
The patient does not agree There are not enough anesthetic and resuscitation facilities The technician is not proficient in the technique.
3. Procedure for endotracheal anesthesia for endotracheal bypass to break the floor of the ventricles
Before conducting endotracheal anesthesia, the doctor will examine the anesthesia before surgery to detect and prevent risks, explain to the patient and cooperate. Evaluation of difficult intubation. In some cases, patients were given sedation the night before surgery.Perform the technique:
Position: Lie on your back, breathe 100% oxygen 3-6 l/min at least 5 minutes before induction of anesthesia. Install a Monitor Set up an effective transmission line. Pre-anesthesia (if necessary) Induction of anesthesia Intubation: There are two techniques of intubation: Oral intubation and nasal intubation Maintenance of anesthesia.
4. Some complications may be encountered when performing endotracheal anesthesia
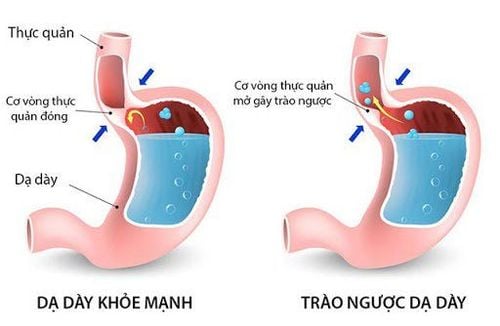
Trào ngược dịch dạ dày vào đường thở
4.3 Incident due to intubation Failure to intubate: Handle according to endotracheal intubation procedure difficult trachea or switch to another method of anesthesia.
Biến chứng sau rút ống nội khí quản có thể gặp như đau họng
4.5. Complications after extubation Respiratory failure after extubation due to various causes Sore throat hoarse voice Vocal - tracheobronchial spasm Upper respiratory tract laryngotracheal stenosis. Dr. Ngat has more than 15 years of experience as an Anesthesiologist and resuscitator at Hospitals: Da Nang Obstetrics and Gynecology Hospital, Hospital 199 of the Ministry of Public Security, Tam Tri Hospital in Da Nang. Currently, he is an anesthesiologist at the Department of General Surgery - Vinmec Da Nang International General Hospital.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
SEE MORE
Laparoscopic surgery to break the floor of the third ventricle Learn about testing cerebrospinal fluid to find the cause of headaches Dangerous complications of hydrocephalus