This is an automatically translated article.
The article was professionally consulted with Specialist Doctor II Dinh Van Loc - Department of General Surgery - Vinmec Danang International General Hospital.The tonsils are lymphatic organs located on both sides of the throat that are responsible for protecting the child's body against the invasion of harmful microorganisms through the respiratory and digestive tracts. Many children with tonsillitis are often prescribed tonsillectomy to limit tonsillitis complications such as difficulty breathing, snoring, repeated infections. The purpose of tonsillectomy in children is to remove the entire inflamed or hyperplastic tonsil tissue in the oropharynx.
1. Indications and contraindications for endotracheal anesthesia for tonsillectomy in children
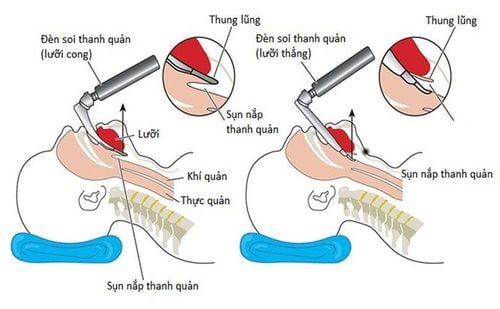
Tonsillectomy in children under endotracheal anesthesia is a surgical method performed under general anesthesia using an endotracheal tube to control the airways of the child. Children with tonsillitis are indicated for surgery under anaesthesia in cases where it is difficult for young children to cooperate or in cases of complicated surgical prognosis with many complications. Some cases in which endotracheal anesthesia cannot be performed in tonsillectomy in children include:Medical facilities do not guarantee facilities or do not have enough means and tools to use in endotracheal anesthesia Anesthesiologists have not been trained and experienced in performing endotracheal anesthesia In case the patient or patient's family does not agree to perform the technique. Children suffering from acute respiratory infection syndrome (Need to be stabilized before surgery)

Gây mê nội khí quản cắt amidan được chỉ định trong trường hợp tiên lượng phẫu thuật phức tạp
2. Procedure for performing endotracheal anesthesia to remove tonsils in children
The procedure of performing endotracheal anesthesia for tonsillectomy in children should be strictly followed by the following steps to ensure the safety and effectiveness of the surgery:Preparation of instruments and tools: including: including monitoring of patient's vital signs (heart rate, respiratory rate, blood pressure, temperature, oxygen saturation, ... ), ventilator, sputum aspirator, endotracheal tube of various sizes size, laryngoscope, mask, canule, and instruments used in tonsillectomy in children such as electric knife, cold knife, forceps, needle, suture... Treatment requires a thorough clinical examination, history and history before performing endotracheal anesthesia for tonsillectomy in children to rule out contraindications. The steps in the procedure as well as possible complications also need to be consulted and explained before anesthesia in order to have good consensus and cooperation between medical staff and the patient and patient's family. core. All cases require evaluation and classification of difficult intubation to follow through with difficult intubation procedures or alternative anesthetic options. Have the patient lie on the operating table in the supine position. Find and place a large peripheral intravenous line.

Kỹ thuật thực hiện gây mê nội khí quản cắt amidan ở trẻ em
End of anesthetic effect, analgesia, muscle relaxant (TOF > 0.9.) Patient awake, following orders (open eyes, open mouth, sticks out tongue, clenched fists, lifts upper head) 5 seconds) Deep breathing spontaneously, normal breathing rate according to age, Vt >6ml/kg SaO2 98-100% Pulse, stable blood pressure. Body temperature > 36.50 C. No BC of anesthesia and surgery.
3. Monitoring and detecting complications after tonsillectomy in children
Monitor postoperative careGive oxygen through the nose Monitor heart rate, Spo2, breathing rate, blood pressure, temperature. Monitor bleeding after surgery: is most important Pay attention to patient lying on one side, head low. Postoperative analgesia: Paracetamol, ibuprofen Prophylaxis of vomiting: ondansetron, dexamethasone. Tonsillectomy in children with endotracheal anaesthesia may have some of the following complications:
Failure to intubate: need to be managed in the direction of difficult intubation or alternative anesthetic methods. . Trauma when intubation: possible injuries are broken teeth, bleeding, trauma to the tongue, trauma to the vocal cords, foreign bodies in the airway. Treatment depends on each specific case. Incorrect position of the endotracheal tube: during surgery, the endotracheal tube may fall deep inside or fall out or bend the tube, causing difficulty in breathing. If this accident occurs, it is necessary to find the cause and provide emergency treatment to protect the airway and ensure the patient's breathing. After extubation, the patient may face situations such as respiratory failure, laryngospasm, hoarseness or loss of voice, upper respiratory tract infection, pneumonia, ... Reflux Ingestion into the respiratory tract: emergency management should be carried out by aspirating gastric juice from the respiratory tract while placing the patient in a position of low head tilted to the side. The endotracheal tube needs to be repositioned quickly to control the airway. After surgery, the patient should be examined and monitored to detect early complications of aspiration pneumonia, if any.

Trẻ có thể bị suy hô hấp sau khi rút ống nội khí quản
Vinmec Health System is also proud to be the first hospital in Vietnam to sign with the World Anesthesiology Association (WFSA) towards the goal of becoming the safest hospital for surgical anesthesia in Southeast Asia. We always apply advanced anesthetic and analgesia techniques, apply strict and routine procedures and standards to ensure high safety for patients.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.