This is an automatically translated article.
Posted by Specialist Doctor II Nguyen Thi Hoai Nam - Head of Pain Relief Unit - Department of Surgical Anesthesia - Vinmec Central Park International Hospital
Endotracheal intubation is a good and effective method of airway control. However, endotracheal intubation can cause dangerous, even life-threatening complications, so there should be standard technical procedures and close monitoring.
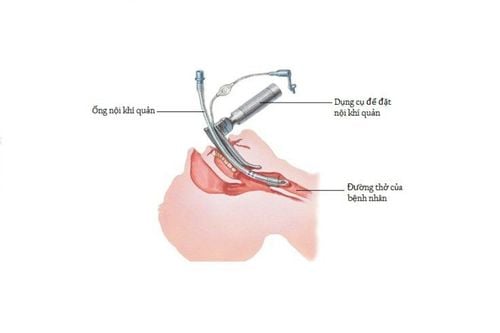
1. What is intubation?
Endotracheal intubation is the procedure of inserting a tube through the nose or mouth, through the larynx so that one end of the catheter is in the patient's windpipe. The purpose of intubation is to ensure ventilation and control the airway. Intubation is usually indicated when the patient is unable to breathe on their own, needs help with breathing or during endotracheal anesthesia. This is a procedure that requires fast, accurate performance to ensure patient safety. Therefore, the person performing the procedure must be trained and experienced, especially in the case of an emergency or difficult airway, which can cause many serious complications.
Currently, endotracheal intubation is the best and most effective method of airway control. However, endotracheal intubation and extubation can cause dangerous, even life-threatening complications. Therefore, it is necessary to have standard technical procedures and to be closely monitored when performing the procedure. In addition, this is also an invasive procedure when performed on patients requiring the consent of the patient or family. Before performing the procedure, the doctor needs to explain the benefits as well as the possible complications, and at the same time let the patient or family sign an agreement to perform the procedure.
2. Indication for intubation in which case?
2.1. Benefits of intubation
Control and maintain airways Provide high-concentration oxygen Ventilate mechanically Suction viscous sputum and secretions and help prevent aspiration of secretions from the stomach, throat, mouth, or upper respiratory tract in the event of a decrease or loss of the patient's airway. awareness. Use emergency medicine, resuscitation when there is no transmission line2.2. Indications for endotracheal intubation
Emergency:
Acute airway obstruction due to trauma, foreign body, upper airway burn, laryngospasm or edema... Loss of protective airway reflexes due to disturbances in consciousness due to trauma, drug overdose, cerebrovascular accident... Respiratory failure, hypoxemia, increased CO2 Cardiac arrest, apnea Coma Coma Bilateral jaw fracture Heavy bleeding into the oral cavity due to tumor or trauma Anesthesia Anesthesia endotracheal intubation: in case of surgery requiring general anesthesia.

Bệnh nhân hôn mê được chỉ định đặt nội khí quản
3. Possible complications when intubation
3.1. Instant Catastrophe
Accidents caused by stimulation: Rapid pulse, increased blood pressure Slow pulse, cardiac arrest due to parasympathetic stimulation Strokes due to injury: tearing of lips, broken teeth, tearing of tongue, perforation of trachea, esophagus. Swollen larynx causes difficulty breathing, lack of oxygen Vomiting, aspiration of vomit into the lungs causes Mendelson syndrome (aspiration pneumonia), usually occurs when the patient has a full stomach. Atelectasis due to tube insertion too deep into the bronchus, often into the right bronchus, causing left lung atelectasis Lung infection due to failure to respect the principle of aseptic, introducing bacteria from the outside into the lungs Tracheospasm due to irritation Placed in food Management: If not detected in time, it can cause irreversible brain damage (brain death) or death due to lack of oxygen. Obstruction of endotracheal tube due to foreign body or collapsing tube, flexion of the larynx. Vocal cord paralysis due to recurrent nerve damage. Intubation is not possible because the patient has a difficult airway. This is a serious complication that can lead to death due to uncontrolled airway. Endotracheal intubation or tube deviation due to improper fixation or the patient's stimulation to struggle.
3.2. Long-term complications
Painful swallowing, difficulty swallowing or hoarseness due to damage to pharynx, larynx, usually after 5-7 days Granulomas, papillomas in vocal cords cause persistent hoarseness Tracheal stenosis: due to balloon insertion of endotracheal tube Too much tension for a long time causes compression and damage, necrosis of the mucosa causing scarring, narrowing of the trachea

Đặt ống nội khí quản có thể gây khàn tiếng
4. Extubation of endotracheal tube
When the patient is awake, in the case of endotracheal anesthesia, the tube can be withdrawn while the patient is still anesthetized but has reflexes and sensations in the pharynx and larynx. On the other hand, when the patient's respiratory system is stable, breathing is regular, breathing is normal, breathing volume is sufficient, and muscle relaxants have worn off, they can also be evaluated for extubation.
In addition, when the circulation is stable, the pulse and blood pressure are normal. Oxygen saturation (SpO2) within the normal range can perform extubation.
5. What to do when extubating
To minimize complications after extubation, technicians and doctors need to consider the following factors:
Check if the patient is eligible for extubation. Prepare enough instruments for re-intubation if necessary Remove mucus from the endotracheal tube and in the patient's mouth Give oxygen 3-5 minutes Deflate the balloon Gently remove the tube Give oxygen through a mask or nose Monitor vital signs signal during and after extubation.

Rút nội khí quản cần rút ống nhẹ nhàng
6. What can be done to minimize complications during intubation?
The person performing the procedure is trained and experienced Fully equipped with first aid equipment and tools for airways and difficult airway management Fully equipped to monitor the patient's vital signs Equipped with measuring cables ETCO2 (end-expiratory CO2 concentration): the gold standard for determining whether the endotracheal tube has entered the correct trachea. Follow the correct technique, insert and withdraw the tube gently, avoiding injury. Decrease the excitatory reflex during intubation by administering sedation, anesthesia, analgesia, muscle relaxants, anesthesia, or intubation at an appropriate level of anesthesia if endotracheal anaesthesia Sellick's maneuver (cricoid compression) ) when intubating patients with a full stomach to avoid aspiration and prevent Mendelson's syndrome. Proper endotracheal care: ensure sterility when aspirating sputum, endotracheal balloon pressure 20-30cmH2O, check balloon pressure twice a day, intermittently deflate the balloon to avoid causing ischemia of the tracheal mucosa causing scarring tracheal stenosis. Closely monitor, detect blockages, clogged pipes, drop pipes for timely handling. Intubation is a simple procedure, easy to perform but extremely important, if you encounter small mistakes, it can also leave dangerous complications after extubation. Therefore, patients should choose reputable addresses with good expertise to perform this procedure.
Vinmec International General Hospital has applied the technique of endotracheal intubation during emergency, surgical treatment of diseases. The technique of endotracheal intubation at Vinmec is performed methodically and in accordance with standard procedures by a team of highly qualified medical professionals and modern machinery. From there, bring the optimal treatment effect for customers! If you have a need for medical examination by modern and highly effective methods at Vinmec, please register here.