This is an automatically translated article.
The article is professionally consulted by Master. BSCK II Phan Thi Minh Huong - Gastroenterologist - Department of Medical Examination & Internal Medicine - Vinmec Da Nang International General Hospital.Peptic ulcer is the leading cause of gastrointestinal bleeding, accounting for 40-45% of all types of gastrointestinal bleeding. Although the disease can be treated with drugs, it can easily lead to serious complications, even a mortality rate of up to 10%.
1. Gastrointestinal bleeding site
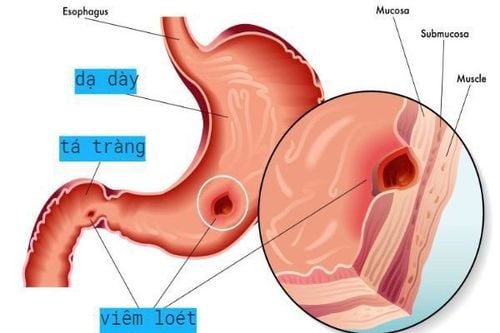
Gastrointestinal bleeding often occurs in the following locations:Gastric ulcer: usually originates in the small curvature of the stomach, the back of the stomach and the cardia. 15 - 16% of gastric ulcers will have bleeding complications. The ulcers are fibrous, perforating the tissues around the ulcer site and gastric blood vessels, causing gastric bleeding. Duodenal ulcer: common in the duodenal bulb, rarely in the duodenal segment. Ulcers are usually on the anterior, posterior, and superior margins. Many fibrous ulcers cause the duodenal bulb to deform, the ulcer penetrates into the duodenal wall, causing bleeding. 25% of duodenal ulcers have bleeding complications. Duodenal ulcers are more common than gastric ulcers. Bleeding from gastric mucosa: there may be no ulcerative lesions. The cause is acute inflammation or the effect of non-steroid anti-inflammatory drugs, corticosteroids causing sudden ulcers. Bleeding from the gastric mucosa may be present in a few spots or bleeding from the entire gastric mucosa.
2. Manifestations of bleeding lesions
Ulcers that penetrate into blood vessels: Ulcers located near the major arteries of the stomach and duodenum are often capable of perforating blood vessels such as: ulcers located near the splenic artery, the pyloric artery (marginal ulceration). small curvature of the stomach, ulcers on the back of the stomach...), ulcers near the gastroduodenal artery (lower border ulcers, upper border ulcers, posterior duodenal ulcers...). These ulcers are very easy to lead to complications that cause severe bleeding. If the emergency endoscopy can see the blood vessels are bleeding. Bleeding from the blood vessels of the bottom of the ulcer: The ulcer penetrates the wall of the stomach and duodenum, causing damage to the blood vessels. Bleeding from the blood vessels of the base of the ulcer is not as intense as when bleeding from the ulcer eats into the blood vessel mentioned above, but it is very easy to recur, repeated many times. Treatment may cause the ulcer to stabilize temporarily. If the endoscope can see the bottom of the ulcer, stop bleeding, but it is very likely that the tip of the whole blood vessel is raised. Bleeding at the edge of the ulcer: Caused by the development of the ulcer, the ulcer's mucosal edge is inflamed, causing bleeding. Bleeding at the edge of the ulcer is usually small, does not cause massive bleeding, but is persistent. If the endoscopy can see the edge of the ulcer is swollen, dark red and bleeding.3. Notes when taking medical history in treatment
People with stomach and duodenal ulcers for many years. May have had medical treatment and diagnosed by X-ray but there are no signs of stomach and duodenal disease. The patient suddenly had symptoms such as passing dark black stools, vomiting blood... The patient had a history of gastrointestinal bleeding due to gastric and duodenal ulcers many times, had medical treatment. , has stopped bleeding and is stable, but if the patient is admitted to the hospital with bleeding, it can be clinically identified as gastrointestinal bleeding due to gastric and duodenal ulcers. Patients with no history of gastric and duodenal ulcers: patients will have signs of bleeding, the ulcers progress silently and lead to bleeding complications.
Bệnh nhân đã có tiền sử bị xuất huyết tiêu hóa do loét dạ dày
4. Symptoms of gastrointestinal bleeding due to gastric and duodenal ulcers
4.1. Functional symptoms Nausea, vomiting blood: The patient has a feeling of fullness, discomfort, nausea, accompanied by a fishy taste in the mouth. The patient vomits blood, there may be food in the blood. Severe vomiting of fresh blood is usually caused by a stomach ulcer. If vomiting blood is black, it is usually due to a duodenal ulcer. Black stools: The patient passes stools that are black like coffee grounds. The stools are viscous and have a very unpleasant stench. Symptoms of black stools usually appear right after the patient vomits blood. Abdominal pain: Patient has dull, burning pain in the upper navel area. Symptoms of abdominal pain may appear several days before bleeding. 4.2. Systemic symptoms Dizziness, dizziness, lightheadedness due to anemia after vomiting blood. The patient may faint or go into shock. Accompanied by the following symptoms: pale skin, pale skin, sweating, tinnitus, thirst Rapid pulse > 90 times/minute Arterial blood pressure drops sharply, possibly below 80 mmHg If the patient is bleeding from If there is little or no bleeding, the symptoms of blood loss shock will be mild or absent. 4.3. Physical symptoms There are no obvious signs, can see pain in the abdomen above the navel, signs of the stomach and duodenum are rarely specific No palpable lump, liver and spleen are not enlarged On examination The rectum shows black stools, no fresh blood and lumps5. Laboratory tests
5.1. Endoscopy Endoscopy is the most important diagnostic method when determining gastrointestinal bleeding due to gastric and duodenal ulcers. Endoscopic methods can help determine the cause of bleeding, the exact location of bleeding. The ability to identify lesions with accuracy up to 95%. In addition, endoscopy can help control bleeding through sclerotherapy, electrocautery, laser... In the first 24 - 72 hours of emergency, endoscopic can be performed.5.2. Tests Some basic tests need to be done to assess the level of blood loss of the body such as:
Test of red blood cell count, white blood cell count Hematocrit test Hematocrit test, platelet prothrombin ratio Group test blood... In addition, a number of tests are performed to assess the general condition and make a differential diagnosis.
5.3. Ultrasound In order to determine whether the cause of bleeding is due to peptic ulcer or not and detect co-morbidities such as hepatitis, cirrhosis, obstructive jaundice, etc., ultrasound can be used.
6. Diagnosis

Chẩn đoán viêm loét dạ dày tá tràng
Clinical signs of upper gastrointestinal bleeding Patients with repeated bleeding Patients with a history of gastric and duodenal ulcers Patients with symptoms of other diseases Old radiographs show gastric and duodenal ulcers Endoscopy determined the cause of bleeding was from gastric and duodenal ulcers 6.2. Differential diagnosis Differential diagnosis of bleeding due to peptic ulcer or bleeding from other diseases such as:
Bleeding due to gastric cancer Bleeding due to rupture of esophageal varices, stomach Biliary tract bleeding ... To accurately determine the health status, patients with one of the above signs should see a doctor. Vinmec International General Hospital with comprehensive expertise, services and facilities will help patients have a safe and comfortable experience when visiting Vinmec.
Doctor Huong has over 30 years of experience in the field of Gastroenterology in which with nearly 20 years holding the position of Deputy Department, Head of Department of Hue Central Hospital. Currently, he is a Doctor of Gastroenterology - Gastrointestinal Endoscopy - General Internal Medicine Department of Vinmec Da Nang International General Hospital.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.