This is an automatically translated article.
The article is professionally consulted by Master, Doctor Vu Huy Binh - Department of Medical Examination & Internal Medicine - Vinmec Hai Phong International General Hospital.Duodenal injury is a rare lesion in abdominal trauma, accounting for only about 3-5% of traumatic abdominal injuries and is often associated with pancreatic rupture.
1. Types of duodenal trauma
Injuries to the duodenum are common injuries caused by traffic accidents, work accidents, or in daily life, due to stabbings, shootings, etc. The pancreas and duodenum are two organs located next to each other, close to each other. anterior to the spine and to the retroperitoneum. Therefore, they are easily injured together, especially in the case of severe blunt trauma to the abdomen and spine.1.1 Intraperitoneal duodenal rupture Flooding with digestive juices, intra-abdominal bile, lesions often have rough margins, surrounding crushed tissue is larger than the lesions seen on the duodenal wall, blood can be seen Large subserosal accumulation around the lesion and spread to adjacent organs, especially the head of the pancreas
The abdominal cavity often has little clear yellow fluid due to the reaction of the peritoneum. Often seen a large retroperitoneal hematoma, sometimes spreading to the iliac fossa (P), in the lesion, digestive juices are often seen, sometimes including gas. The roots of the transverse mesenteric colon have green marks due to bile stasis, which is the best sign to detect duodenal rupture at surgery.
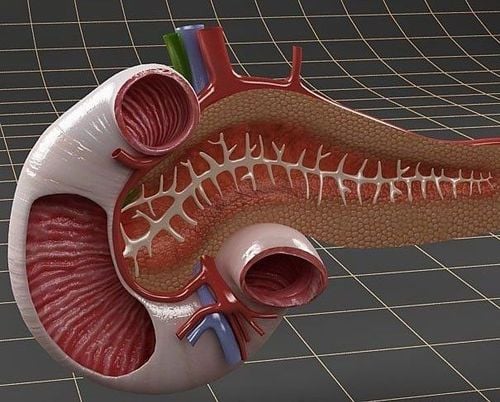
Hình ảnh tá tràng trong cơ thể
Anatomical classification of duodenal trauma
Grade I: Serological tear, hematoma or contusion, no perforation. Grade II: Complete tear of the duodenum, the pancreas is not damaged. Grade III: Any of the above 2 degrees, associated with minimal trauma to the pancreas: contusion, hematoma, tear but the pancreatic duct is not injured. Grade IV: Severe damage to the head of the pancreas and duodenum combined.
2. Diagnosis of duodenal injury
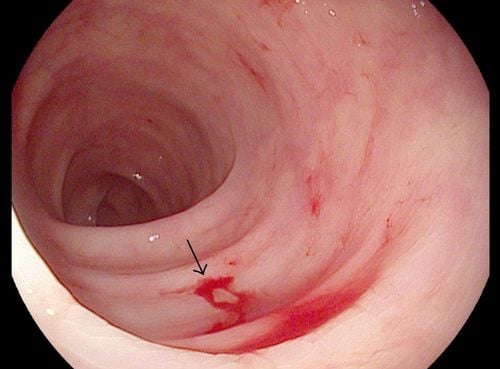
2.1 Functional symptoms Abdominal pain after trauma Constipation and defecation Mild dyspnea If late arrival with obvious signs of infection, high fever 39-40 degrees Celsius 2.2 Physical symptoms Bruised abdominal wall Abdominal stiffness like wood, loss of area Pre-hepatic opacities similar to gastric perforation Peritoneal palpation (+) Rectal examination of pouch with Douglas bulging pain 2.3 Subclinical Blood tests: Leukocytosis Abdominal X-ray unprepared with air sickle Abdominal ultrasound has Free fluid CT scan of the abdomen with contrast to evaluate other lesions if present in the abdomen accompanied by Laparoscopy with digestive juices or BC >500/mm3
Chẩn đoán chấn thương tá tràng bằng các phương pháp hình ảnh
3. Methods of treatment of duodenal injury
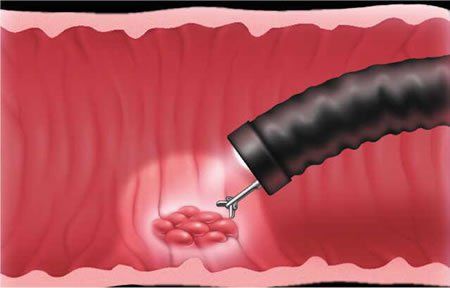
3.1 Principles of treatment Indication for emergency surgery: endotracheal anesthesia Use systemic antibiotics at the time of induction of anesthesia Wide mid-upper-under-umbilicus incision Investigate lesions with the principle: All visceral organs in the abdomen . In a certain order. Mark each time an injury is found, continue to search until all organs are viewed. Evaluate the damage and then choose the most optimal treatment with the goal: Prioritize saving the patient's life. The more complicated the injury, the more severe the patient is, the more gentle and simple the treatment will be, treating sequelae if the patient lives. 3.2 Methods of treatment of duodenal injury There are two methods of surgical treatment of duodenal injury: conservative treatment and resection treatment3.2.1 Duodenal-conserving surgery For lesions causing only lower hematoma serosa, submucosal or duodenal serosa tear, just suture the torn serosa or remove the hematoma, taking care not to perforate the duodenum
For grade II, III lesions, the following methods can be chosen The following surgical methods:
Suture only for sharp, compact, not crushed wounds, should drain the gallbladder to reduce pressure Suture with protective surgery: Connect 1 loop of intestine to the wound = grade IV = AAST : when the duodenal wound is wide, loses many tissues, if sutures can cause narrowing or lesions that expose the ampulla of Vater wide, a loop of jejunum can be inserted into the wound (Y-shape) after having Clean resection of crushed tissue For wounds in D4 : It is possible to cut the duodenojejunal angle and make an anastomosis of the duodenum to the healthy tissue.

Tùy tình hình bệnh nhân để bác sĩ chỉ định phương pháp phẫu thuật phù hợp
Pancreatectomy Colon Total pancreaticoduodenectomy.
4. Possible complications after surgery and treatment direction
If the lesions are treated early, including retroperitoneal lesions, postoperative progress is usually favorable. Complications such as: Leakage or rupture of duodenal suture usually occurs on the 3-5th postoperative day, Patients have symptoms of fever, abdominal pain, catheter to drain the abdomen to bile, if the fistula is localized, conservative treatment is by continuous suction through the abdominal tube, water and electrolyte replacement For general peritonitis, treatment must be performed. reoperation, these cases are often severe, with a high mortality rate due to infection.Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.