This is an automatically translated article.
The article was written by Doctor Mai Vien Phuong - Department of Medical Examination & Internal Medicine - Vinmec Central Park International General HospitalWith the development of gastrointestinal endoscopy, a number of recent studies have shown that cirrhosis is associated with the development and progression of portal hypertension. In addition to the main picture of portal hypertension commonly seen on endoscopic examination of mucosal mosaicism, erosive lesions have also been detected in the stomach of cirrhotic patients and have been classified by some authors as a form of portal hypertension.
1. Definition and classification of portal hypertension
With the development of endoscopy, gastric lesions in cirrhotic patients have been reported. First McCormack T.T. introduced the concept of edematous gastritis in gastroscopy of cirrhotic patients. However, in the process of finding out, McCormack T.T. found very few inflammatory cells in the histological image of gastric mucosa. He suggested renaming it edematous stomach disease.Until now, there are still quite a few definitions of portal hypertensive gastropathy (BDDTAC). Similarly, the classification of portal hypertension is still not consistent, focusing on 2 groups:
The group is divided into two types: Mild, severe according to the classification of McCormack T.T., Baveno III. Group 3 types: Light, medium, heavy according to the classification of Tanoue K. and NIEC. Although both groups of classification methods do not have optimal accuracy and practicality, the two classification methods still have more advantages due to having more consensus among endoscopists. In the group that divides BDDTAC into two categories, the Baveno III classification is the most widely accepted and used.
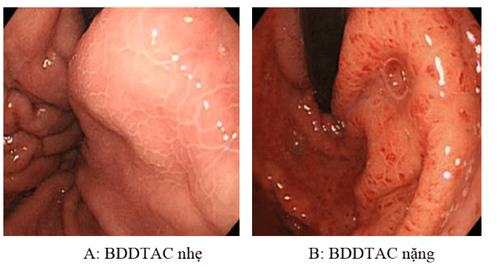
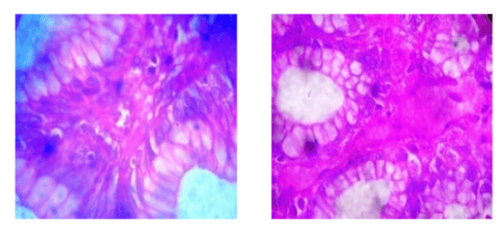
Hình ảnh bệnh nhân bị bệnh lý dạ dày tăng áp cửa
2. Pathology of portal hypertension
According to a study by Barakat M. with the results of histopathological imaging studies of over 133 gastric biopsy samples of patients with BDDTAC images, the author found that edema of the gastric mucosa is common. The most (116 samples, accounting for 87.2%), there was no statistically significant difference between severe and mild BDDTAC. Also according to Barakat M., gastric mucosal microvascular dilation was also the second most common with significantly higher incidence (p < 0.01) in the group of patients with severe versus mild BDDTAC. According to Lash R.H., gastric microvascular dilation is usually located in the submucosa but can also occur in the mucosal layer.
This image is more common in the body region than in the antrum. One possible picture in BDDTAC is the appearance of vascular neoplasia under the influence of portal hypertension on vascular endothelial growth factor VEGF. Less common is fibrinolysis with increased fibrosis.
On the other hand, in a study by Misra V. and CS on measuring lumen diameter and mucosal capillary wall thickness in cavernous and gastric aneurysms on cirrhotic patients, the author found wall thickness Capillaries in the trunk and gastric aneurysm increased significantly compared to normal subjects while the lumen diameter increased significantly only in the antrum region. This study also shows that capillary wall thickness is more valuable than measuring lumen diameter in the diagnosis of portal hypertension.
In addition, Toyonaga A. found many shunts connecting capillary veins and arteries in the lower gastric mucosa through microangiography. In addition to the images of dilated and stagnant blood vessels, the ducts are often hyperplastic and zigzag. The connective tissue between the ducts has small areas of hemorrhage, fibrous tissue, scattered with neutrophils, but more commonly, lymphocytes and macrophages are present. There is no or very little inflammatory cell imaging in BDDTAC. In the study of Barakat M., only 3/133 (2.3%) biopsy samples had dense presence of inflammatory cells.
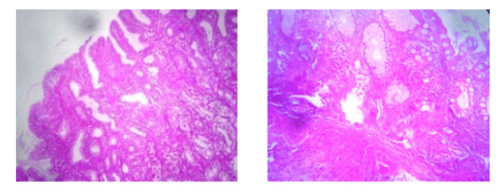
Hình ảnh thân vị phù nề, mạch máu thân vị dãn, đặc trưng của bệnh lý dạ dày tăng áp cửa
3. How is this imaging specific for portal hypertension?
The histopathologic picture of BDDTAC is not specific for the diagnosis of BDDTAC because these features can be present in other gastric conditions, especially chronic H.P. gastritis and reactive gastritis. reactions to drugs, acids, or bile. Therefore, histopathological image is only a contributing factor besides the main clinical and endoscopic factors for the diagnosis of BDDTAC.
Hình ảnh mạch máu tăng sinh và viêm xơ hang vị ở bệnh dạ
4. Distribution and severity of endoscopic portal hypertension
Some studies show that BDDTAC images appear mainly in the body (89.2%) and gastric aneurysm (90.2%) compared to the antrum (4.9%). According to the study of Iwao T. also showed that the frequency of occurrence of BDDTAC in the body and gastric aneurysm was higher than in the antrum (p < 0.01).
This may be because the structure of the vascular system of the body and gastric aneurysm has many things in common: The left gastric vein has a rather large size in charge of carrying blood from the esophageal vein, the gastric aneurysm body area drains directly into the vein. door circuit. The left gastric vein, together with the short gastric vein and the left gastric omentum vein, forms a vascular system that covers the body and the gastric aneurysm.
A special feature of the portal vein system is that there is no valve, so when there is increased pressure in the portal vein, the pressure will directly affect the blood vessels attached, causing an increase in pressure. within that vascular system and dilate the vessels, contributing to the formation of BDDTAC.
In contrast, the pyloric antrum is mainly responsible for the gastric vein. This is a small blood vessel that zigzags before emptying into the portal vein, so portal hypertension will not have much impact on the pyloric antrum and cause less vasodilation, less BDDTAC image.
Vinmec International General Hospital is a prestigious address trusted by many patients in performing diagnostic techniques for digestive diseases, hepatobiliary diseases, portal hypertension, cirrhosis... Along with At that time, at Vinmec Hospital, screening for gastric diseases was done through gastroscopy with Olympus CV 190 endoscope, with NBI (Narrow Banding Imaging) function for The imaging results of mucosal pathology analysis are clearer than conventional endoscopy, detecting atrophic gastritis lesions, intestinal metaplasia, low-grade, high-grade gastric dysplasia, and lesions. Inflammation and edema due to portal hypertension... Vinmec Hospital with modern facilities and equipment and a team of experienced specialists, always dedicated to medical examination and treatment, customers can peace of mind with gastroscopy and esophagoscopy services at Vinmec International General Hospital.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
References
Nguyen Xuan Hien (2009), “Research on endoscopic images of esophageal mucosa in cirrhosis patients”, Vietnam Journal of Gastroenterology, p. 1075-1079. Tran Van Huy (2006), "Efficacy of endoscopic rubber band ligation combined with propranolol in preventing recurrence of esophageal varices in cirrhosis patients", Vietnamese Medicine, Hepatobiliary Topics, p. 140-149 Study on the efficacy of esophageal varices ligation in combination with propranolol in preventing recurrent bleeding and its impact on portal hypertension due to cirrhosis (2014). Tran Pham Chi, Doctor of Medicine Thesis, Hue University of Medicine and Pharmacy Nguyen Ngoc Thanh, Nguyen Thuy Oanh (2012), "Evaluate the effectiveness of methods to prevent recurrent esophageal varices rupture by elastic ligation combined with propranolol. , Journal of Medicine Ho Chi Minh City, 16 (3), p. 29-35.