This is an automatically translated article.
Article written by Master, Doctor Mai Vien Phuong - Gastrointestinal endoscopist - Department of Examination & Internal Medicine - Vinmec Central Park International General Hospital
Gastrointestinal stromal tumor (GIST) is a rare tumor of gastrointestinal origin. From the onset, the disease sometimes silently shows no symptoms, but sometimes causes the patient's health to deteriorate, metastasize to adjacent organs quickly.
1. What is a gastrointestinal stromal tumor?
Gastrointestinal stromal tumors (GISTs) are soft tissue sarcomas, ie neoplasms arising from the mesenchymal layer of the body. The disease mainly occurs in middle-aged and elderly people, rarely in young people.
Gastrointestinal stromal tumors can be benign or malignant. In particular, benign tumors account for 70-80% of the majority, found in the stomach, small intestine, esophagus, colon and rectum. Tumors with high malignant potential are usually >5 cm large, epithelial cells, and can metastasize to the liver and peritoneum.
2. Characteristics of gastrointestinal stromal tumors
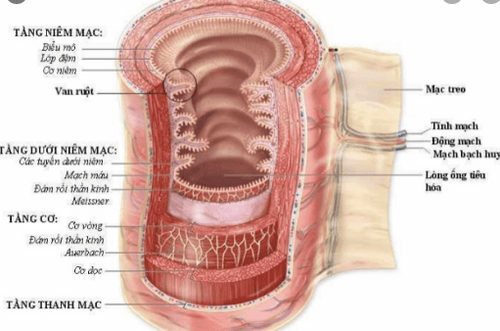
Cấu tạo thành ống tiêu hoá – U dưới niêm là những cấu trúc nằm dưới lớp niêm mạc
Gastrointestinal stromal tumors may occur elsewhere in the gastrointestinal tract. These are submucosal lesions ranging in size from 1 cm to 40 cm in diameter. Approximately 50-70% of gastrointestinal stromal tumors arise from the stomach. From the jejunum is 20-30%. Rarer are from colon and rectum (5-15%) and esophagus (<5%). Very rarely occurs outside the gastrointestinal tract, such as in the pancreas, the greater omentum, the mesentery of the small intestine or the peritoneal cavity.
3. Signs of gastrointestinal stromal tumor
Clinical symptoms may include:
Ambiguous, nonspecific abdominal pain or discomfort (most common) Early loss of appetite or feeling of fullness Feeling of abdominal mass (rare) Shortness of breath Systemic symptoms: Fatigue, anorexia, weight loss and symptoms of metastasis (common disease metastasizes by blood into the liver, peritoneum...). Signs of intestinal obstruction and symptoms may be specific to the following sites: Esophageal Esophagitis: Difficulty Swallowing Gastrointestinal tract: Constipation and abdominal distension, Blood in stools Gastrointestinal tract: Jaundice: Jaundice , bowel obstruction
4. Diagnosis of gastrointestinal stromal tumor
When there are signs and symptoms suggestive of a CRC, investigations should be done to determine the site of co-metastasis to other organs. Specifically, these include:
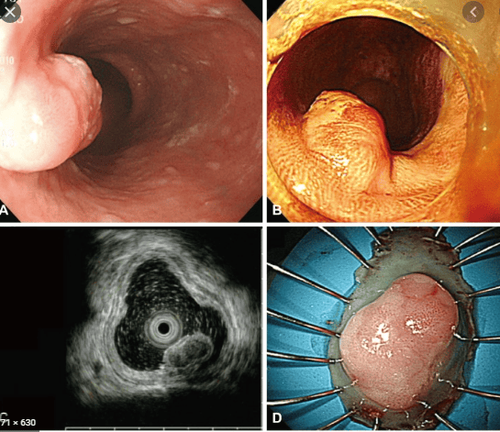
Contrast tomography: Take a contrast agent to better see the stomach and small intestine when taking X-rays. Or inject contrast. Helps assess the size and location of the tumor. Upper gastrointestinal endoscopy: esophagus, stomach, first small intestine. Biopsies of abnormal tissues may be taken. Endoscopic ultrasonography: Endoscopic ultrasound is the most accurate imaging method to evaluate gastrointestinal submucosal tumors because of its ability to individually delineate each layer of the gastrointestinal tract wall and pinpoint the exact location of the tumor. under the mucosa. Fine-needle biopsy: Sometimes these tests are inconclusive or inconclusive. If tumor is still suspected, surgery is needed to remove the tumor and conduct necessary analyzes such as pathology, immunohistochemistry, mitotic index....

Đầu dò siêu âm được tích hợp ở đầu ống soi tiêu hóa.
5. Treatment of gastrointestinal stromal tumors
5.1 Surgery 5.1.1 Endoscopic mucosal resection for gastrointestinal stromal tumors Endoscopic mucosal resection is used to resect mucosal and submucosal tumors up to 2 cm in diameter. Mucosectomy can not only remove submucosal tumors, but also has high diagnostic value.
However, when using this technique, caution should be exercised when cutting tumors originating from the muscle layer because of risks such as: Perforation, bleeding or residual tumor. Therefore, this technique should only be used in the diagnosis and treatment of submucosal tumors originating from the myo-mucosa or submucosa, and should not be used for submucosal tumors originating from the muscular layer or tumors of the duodenum. colon.
5.1.2 Endoscopic submucosal technique Endoscopic submucosal dissection can be used to diagnose and treat submucosal tumors. This technique can be performed for tumors originating from the muscularis or malignant submucosa. Submucosal resection can cut submucosal tumors larger than 2cm, but this is a difficult technique, takes a long time, and has a high risk of complications when the tumor is over 5cm.
Kỹ thuật ESD cắt bỏ u dưới niêm ở thực quản
5.1.3 Endoscopic submucosal endoscopic tumor resection technique Submucosal tunneling was first used in the esophagus to resect the lower esophageal sphincter to treat achalasia. This technique was then used to cut submucosal tumors arising from the muscular layer of the esophagus and cardia.
This technique includes steps: Make a mucosal incision at least 5cm from the lesion, then the bronchoscope is inserted into the submucosal layer and gradually advances to the submucosal tumor, followed by cutting the submucosal tumor by technique Submucosal dissection (ESD) and finally closure of the mucosal incision after complete resection of the tumor.
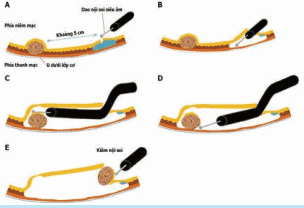
Cắt bỏ u nội soi qua đường hầm dưới niêm mạc
5.2 Imatinib mesylate Adjuvant therapy after complete tumor resection in high-risk cases Neo-adjuvant therapy aims to shrink the tumor prior to surgical resection. 5.3 Tyrosine kinase inhibitors (TKIs) This is a special drug used to treat gastrointestinal stromal tumors by blocking the signals that cause cells to grow. This method is often used for tumors that cannot be removed by surgery or for tumors that need to be reduced before surgery.
6. What is the survival rate of patients with gastrointestinal stromal tumor?
The survival rate in the group with localized primary disease is 5 years and in the group with metastasis or recurrence is about 10-20 months.
Large-sized peptic ulcers are often associated with complications such as: gastrointestinal bleeding, intestinal obstruction and intestinal perforation. Tumors can be classified into high and low risk categories based on size, location, mitotic index, and immunohistochemical test results.
7. Advice for patients diagnosed with gastrointestinal submucosal tumors
GIST tumors in the stomach and colon are larger than 2 cm and are at high risk requiring surgical treatment. Endoscopic ultrasound should be used to diagnose and monitor submucosal tumors (especially submucosal tumors < 2 cm). Asymptomatic leiomyomas do not need to be monitored and treated endoscopically, avoiding waste of time, treatment costs, and risks of diagnostic procedures. Lipomas do not require endoscopic monitoring and treatment unless symptomatic. Submucosal tumors arising from the muscle layer need to be biopsied by fine needle aspiration to determine the nature of the lesion and have an appropriate treatment. Submucosal tumors are potentially malignant and should be removed endoscopically or surgically, depending on the tumor's nature, size, and location. Gastrointestinal cancer screening at Vinmec is a scientific method for early detection of gastrointestinal cancer (esophageal cancer, stomach cancer, colon cancer) and effective treatment regimens.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.