This is an automatically translated article.
The article was professionally consulted with Master, Doctor Le Hong Duong - Anesthesiologist - Department of General Surgery & Anesthesia - Vinmec Hai Phong International General Hospital.In laparoscopic fixation of the rectum and colectomy, endotracheal anesthesia is applied to control the patient's breathing during and after surgery.
1. What is endotracheal anesthesia for fixed rectal surgery, colectomy?
In laparoscopic fixed rectum surgery, laparoscopic colectomy, technique of general anesthesia with intubation, also known as endotracheal anesthesia, is used to control breathing activity. of patients during and after surgery.
2. What preparation is needed for endotracheal anesthesia for laparoscopic rectal fixation, colectomy?
To perform endotracheal anesthesia for laparoscopic rectal surgery, colectomy requires the following means, machinery, equipment, and medications:
The system includes an anesthetic machine (with breathing) , oxygen hand cuffs, monitors of vital functions (such as arterial blood pressure, breathing rate, temperature, ECG, EtCO2, SpO2), suction machine, defibrillator, ... endotracheal tube sizes laryngoscope, laryngoscope, mask, suction tube, oropharyngeal catheter, bulb, soft mandrin, Magill pliers. Salbutamol and Lidocaine 10% spray. Other means of supporting endotracheal anesthesia for endoscopic rectal surgery, endoscopic colectomy, prophylactic colectomy in case of difficult intubation: laryngeal mask, Cook tube, flexible bronchoscope, pliers mouth opener, tracheostomy kit, ...
Mổ nội soi cắt đoạn đại tràng
3. Endotracheal anesthesia procedure laparoscopic rectal surgery, colectomy
Before performing surgery, the patient should be examined under anesthesia to promptly detect and prevent possible risks, as well as evaluate the difficult situation of intubation.
The procedure of endotracheal anesthesia for laparoscopic rectal fixation, colectomy includes the following steps:
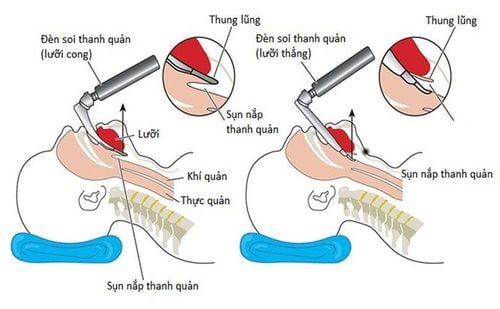
Step 1: Place the patient in a supine position, at least 5 minutes before induction of anesthesia, allow breathing 100% oxygen at a dose of 3 - 6 liters/min. Install machines to monitor and set up transmission lines. If necessary, the patient can be given sedatives from the night before surgery. Step 2: Induction of anesthesia begins with intravenous injection (drugs, etomidate, propofol, ketamine, thiopental, ...), volatile anesthetics (sevoflurane...), analgesics (fentanyl, morphine, fentanyl, .. .), use a muscle relaxant if necessary (rocuronium, succinylcholine, vecuronium, ...). It is necessary to ensure conditions for endotracheal intubation during laparoscopic rectal surgery, laparoscopic colectomy (patients sleep deeply, muscle relaxation is adequate). Step 3: Perform endotracheal intubation. You can choose one of two ways to place it: oral or nasal. The technique of oral intubation is performed as follows: (1) Open the patient's mouth, insert the laryngoscope into the right side of the mouth, move the tongue to the left side of the mouth, insert the light deeply, and combine Use the right hand to press the cricoid cartilage to find the lid and glottis; (2) Perform rapid induction of anesthesia and perform the Sellick maneuver when the stomach is full (as soon as the patient loses consciousness, press the cricoid cartilage 20 - 30 kg until the intubation process is complete); (3) The next step in endotracheal anesthesia for laparoscopic fixation and colectomy is to gently insert the endotracheal tube through the glottis, when the endotracheal balloon passes through the vocal cords about 2 - 3 cm then stop; (4) Gently withdraw the laryngoscope; (5) Intubation of endotracheal balloon; (6) Listen to the lungs, see the EtCO2 index to check that the endotracheal tube is in place; (7) Use adhesive tape to fix the endotracheal tube. In case, if it is necessary to avoid biting the endotracheal tube, the cannula can be placed into the patient's mouth. Step 4: In laparoscopic fixation of rectum, laparoscopic colectomy, in case oral endotracheal intubation is not selected, nasal endotracheal intubation can be carried out as follows: (1) Instill a vasoconstrictor on the side of the nose selected for catheterization; (2) For the nasal passage, choose an endotracheal tube with a smaller size than the oral route; (3) Lubricate the endotracheal tube with lidocaine grease and insert the tube into the nostril. Follow-up steps are similar to oral intubation. However, in unfavorable cases, it is necessary to use Magill pliers to guide the end of the endotracheal tube into the correct glottis, and at the same time, have an auxiliary medical staff push the endotracheal tube in from the outside. Note, apply difficult intubation procedure for difficult intubation cases. Step 5: The next step in anesthesia for endotracheal intubation, laparoscopic rectal fixation, colectomy is to maintain anesthesia with anesthetics (intravenous or vapor), analgesics, and muscle relaxants (if necessary. needed) and control the patient's breathing with a machine or hand squeezer.

Quá trình gây mê tiêu hóa để nội soi cố định trực tràng, cắt đoạn đại tràng
4. Monitoring during endotracheal anaesthesia, laparoscopic rectal surgery, colon resection
During endotracheal anesthesia, laparoscopic rectal fixation surgery, laparoscopic colectomy, the following signs and indicators should be monitored:
Depth of anesthesia: Monitor blood pressure, heart rate , blood pressure, sweating, tearing, BIS, MAC, Entropy (if any) ... Vital signs: Monitor blood pressure, heart rate, body temperature, EtCO2 indicators. SpO2. Monitor in case of wrong position of endotracheal tube, or blocked, folded tube. At the end of endotracheal anesthesia, laparoscopic rectal fixation, colectomy, the following criteria should be met before extubation:
The patient is awake and can follow orders. Breathe spontaneously, breathe evenly, breathing rate is within normal limits. Blood pressure and pulse are stable. Body temperature over 35 degrees Celsius. Raise head >5 seconds, TOF index >0.9 (if any). The patient had no complications from anesthesia and surgery.
Gây mê nội khí quản mổ nội soi cố định trực tràng, cắt đoạn đại tràng
5. Management of complications after endotracheal anesthesia laparoscopic rectal fixation, colectomy
During endotracheal anaesthesia, laparoscopic rectal surgery, laparoscopic colectomy may occur some complications that need to be treated as follows:
Gastrointestinal reflux: When developing Show digestive juices in the oral cavity and airway, immediately aspirate the fluid, place the patient in a low head position and tilt the head to the side. Rapidly intubate the endotracheal tube and remove all fluid from the airway. Monitor patients for lung infections after surgery. Hemodynamic disorders: Depending on the cause and symptoms such as arrhythmia, increase or decrease in blood pressure, ... will be treated appropriately. Difficult endotracheal intubation under anesthesia laparoscopic rectal fixation surgery, laparoscopic colectomy: Switch to difficult endotracheal intubation procedure or proceed with another anesthetic method. Misplaced endotracheal tube into the stomach: Re-intubate the endotracheal tube when misplaced with symptoms of auscultation of the lungs without alveolar murmurs, no measurement of EtCO2. Constriction of the larynx, trachea, bronchi: Complications during endotracheal anesthesia laparoscopic rectal surgery, colectomy may cause difficulty or inability to ventilate. At this time, there will be a crackling sound when listening to the lungs. Or maybe the lungs are dumb. For management, it is necessary to provide adequate oxygen, and at the same time give sleeping pills and muscle relaxants, bronchodilators and corticosteroids to ensure ventilation. In case of respiratory failure, difficult intubation procedure should be applied. Trauma in endotracheal intubation: Depending on the damage such as tooth fracture, bleeding, foreign body in the airway, ... will be treated appropriately. Respiratory complications: Find and treat the cause, ensure ventilation and provide 100% oxygen during endotracheal anesthesia, laparoscopic rectal surgery, laparoscopic colectomy causing respiratory complications such as: The endotracheal tube is folded, retracted or pushed deep into one lung, open or collapsed the respiratory system, the oxygen is exhausted, the effect of soda is gone, causing hypoxia. Complications after extubation: Depending on the cause, choose appropriate management when symptoms appear after extubation such as respiratory failure, hoarseness, sore throat, laryngospasm, gas trachea, bronchi, laryngotracheal and tracheal stenosis, upper respiratory tract infection.

Bệnh nhân có thể suy hô hấp sau phẫu thuật
Endotracheal anesthesia laparoscopic rectal surgery, colectomy can be endotracheal intubation in the nose or mouth. During and after anesthesia, surgery needs to be monitored and promptly treated for possible complications.
Vinmec International General Hospital has applied endotracheal anesthesia technique in examination, diagnosis and treatment of many diseases. The procedure of endotracheal anesthesia at Vinmec is carried out methodically and according to standard procedures by a team of highly skilled doctors and modern machinery. As a result, complications after anesthesia and surgery are always minimized to the maximum extent.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.