This is an automatically translated article.
This article is expertly consulted by Master, Doctor Nguyen Le Duc Hoang - Emergency Medicine Doctor - Emergency Department - Vinmec Danang International Hospital.Intubation is the insertion of an endotracheal tube through the nose or mouth into the trachea. This is by far the best and most effective method of airway control. It is required for the doctor in practice to be proficient in the technique of intubation. There are many methods of intubation where laryngoscope intubation is considered routine.
1. What is emergency intubation?
Emergency endotracheal intubation is a procedure in which a catheter is placed into the trachea to support breathing and perform necessary interventions for the patient. Emergency endotracheal intubation has a number of differences compared to emergency endotracheal intubation (creating an artificial airway for the patient through the cricothyroid membrane, helping to open the airway quickly, especially in case of emergency). acute asphyxiation emergency).Intubation brings many benefits to patients such as:
Maintain airway circulation; Provide oxygen with high concentration to the patient; Provide adequate air volume during artificial ventilation; Facilitating the suction of viscous sputum and secretions; Bringing first aid tools in case the patient has difficulty breathing; Prevent aspiration of secretions from the stomach, throat, mouth or upper respiratory tract; Provide positive pressure at the end of expiration; Isolate the lungs; Creating pathways for the use of drugs in emergency resuscitation. Emergency endotracheal intubation is a simple procedure, easy to practice, and plays a very important role. In case of emergency patients, the procedure of intubation should be performed quickly and promptly, avoiding the risk of complications due to the delay in opening the airway to the patient.

Thiết bị cho hủ thuật đăt nội khí quản cấp cứu
2. Indications/contraindications for endotracheal intubation
2.1 Indications for emergency intubationAcute airway obstruction: Due to trauma, foreign body, infection, upper respiratory tract burn, angioedema, edema, laryngospasm, laryngeal tumor; Loss of protective airway reflexes: In patients with impaired consciousness due to head trauma, drug overdose, cerebrovascular accident, central nervous system infection; Respiratory failure hypoxemia and increased CO2; Circulatory respiratory arrest; Patients with head injury have the following signs: GCS ≤ 8, respiratory failure, loss of protective airway reflexes, spontaneous hyperventilation, dyspnea such as apnea. 2.2 Indications for conventional intubation
Indications for intubation are not immediate, but may be recommended prior to transfer in patients with the following problems:
Bilateral jaw fracture; Heavy bleeding into the mouth or throat cavity; Major convulsions; Significant loss of consciousness. 2.3 Contraindications
There are no contraindications when performing in the emergency room
3. Perform emergency intubation
3.1 PreparationImplementation personnel: Specialist doctors and support team; Prepare the patient: Provide oxygen before intubation; remove dentures (if any); establishment of an intravenous or osseous line; put the patient in a suitable position; assess the possibility of difficult intubation based on anatomy (difficulty tilting the neck, inability to open wide mouth, presence of anatomical abnormalities, upper respiratory tract infection, trauma to the larynx, trachea, facial or head deformity congenital neck,...); Prepare instruments: Surgical kit, endotracheal tube of suitable size, guide rod, laryngoscope, breathing balloon, pre-anesthetic, muscle relaxant,... 3.2 Intubation procedure first aid
Anesthetize the patient, monitor and give oxygen; Lubricate and fix the guide rod in the endotracheal tube; Place the patient's head in a suitable position, open the patient's mouth, gently place the lamp blade into the patient's mouth with correct technique; Observe open glottis, vocal cords, aspirate secretions from airway if necessary; Insert the endotracheal tube, observe as the endotracheal tube passes through the 2 vocal cords; Inflate the endotracheal balloon with 5-10ml of air; Remove the blade from the patient's mouth, hold the endotracheal tube, and withdraw the guide; Connect the balloon to help you breathe into the endotracheal tube; Squeeze the balloon to help you breathe, and at the same time observe the up and down movement of the ribcage; Assess the correct position of the endotracheal tube, fix the tube with a cloth band; Ventilate the patient, continue to monitor the patient's health and position of the endotracheal tube by clinical or flat chest X-ray,... *Note:
With the patient being massaged the external heart thoracic cavity: The interruption of cardiac massage should be minimized as much as possible; In case of failure to intubate within 30 seconds, ventilation should be continued by squeezing the balloon through a mask with 100% oxygen and trying to re-intubate within 20-30 seconds; It is necessary to keep the patient's CpO2 index above 95%; The appropriate depth of the endotracheal tube should be ensured as indicated; Optimal balloon pressure is in the range of 20 - 30 cmH2O.

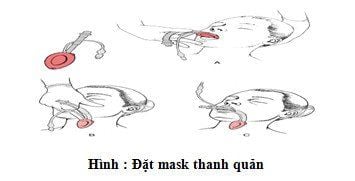
Thực hiện đặt nội khí quản cấp cứu theo quy trình trên
4. Complications
4.1 Complications during intubation:Misplaced tracheal intubation: If not detected in time, the patient may suffer permanent brain damage, even death; Insert the endotracheal tube too deeply, into the right or left main bronchus; Trauma: Tear of lips or tongue, broken or broken tooth, displaced cartilage of funnel, tear of pharynx or trachea, injury of 2 vocal cords (ulcer or loss of function), perforation of esophagus - pharynx, pneumothorax , vomiting and aspiration of gastric juice into the lower respiratory tract, hypertension, tachycardia or arrhythmia, hypotension and bradycardia, increased intracranial pressure,... 4.2 Complications at the site of intubation management
Failed ventilator;
Inhalation into the lungs; Ulcers and granulomas on the vocal cords and in the trachea; Tracheal adhesions; hypoglottic stenosis; Transient vocal cord or nerve paralysis; Formation of the laryngeal membrane; Tracheostomy - esophagus, trachea - carotid artery, trachea - anonymous artery; Tracheal musculoskeletal; Bronchospasm ; Obstruction of the airway due to a problem with the endotracheal tube or from sputum, viscous; The endotracheal tube retracts deeply or slides out due to poor fixation; Injury to the superior laryngeal nerve and the recurrent laryngeal nerve. 4.3 Complications after extubation
Hypoglottic stenosis; Injury to the vocal cords; Hoarseness of voice; Airway ulcers; Sinusitis , otitis media; Necrosis of pharynx, mouth, nose, larynx.
5. Guidelines for monitoring and care after emergency intubation
Endotracheal balloon: Ensure the pressure of 20 - 30 cmH2O, check the pressure twice a day, discharge the balloon for blood circulation (should remove sputum before discharging the balloon); Sputum aspiration: Identify signs of tube blockage or semi-obstruction, monitor suction pressure, increase oxygen 100% before aspiration 2-3 minutes in each sputum aspiration; Check the placement of the endotracheal tube; Monitor SpO2 index; Check the position of the Mayor's tube; Fix the endotracheal tube safely, firmly and change sides to avoid pressure causing ulceration of the oral mucosa; Monitor vital signs (pay attention to breathing); Dental hygiene 2 times / day; Maintain standard patient position: neck straight, no flexion or flexion of the neck; Replace prostheses and adapters every day; Check, replace oxygen catheter in patients receiving oxygen through endotracheal tube; Extubation: Usually done in the morning. The procedure is to check vital signs, prepare instruments for intubation when needed, remove viscous sputum, deflate the balloon, give oxygen to the patient, measure vital signs and closely monitor the patient. the patient's health status. Emergency endotracheal intubation is a good support method for patients in emergencies, anesthesia and surgery. However, this method also has many potential risks affecting the patient's health. Therefore, the patient needs to consult with the doctor, prepare carefully to limit the possible complications when performing this procedure.Master - Doctor Cao Thanh Tam has many years of experience in the diagnosis and treatment of cardiovascular diseases; Performing transthoracic echocardiography in the field of internal medicine and interventional Cardiology; Perform other non-invasive functional investigations in the diagnosis and treatment of cardiovascular diseases. Currently working as a cardiologist at Vinmec Central Park International General Hospital since November 2015.
Customers can directly go to Vinmec Health system nationwide to visit or contact the hotline here for support.
SEE MORE
Things to know when intubation in children Intubation anesthesia cesarean section in patients with preeclampsia Intubation is indicated in what cases?