This is an automatically translated article.
The article was professionally consulted by Specialist Doctor II To Van Thai - Emergency Medicine Doctor - Emergency Resuscitation Department - Vinmec Hai Phong International General Hospital. Thai doctor has more than 34 years of experience in the field of anesthesia - emergency resuscitation.Renal cyst is a benign disease and often has no obvious symptoms. Endotracheal anesthesia for transperitoneal endoscopic renal cyst surgery helps to control breathing during surgery and postoperative resuscitation.
1. Endotracheal anesthesia for transperitoneal endoscopic renal cyst surgery
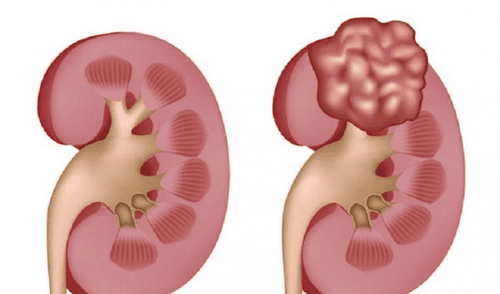
Renal cysts are usually benign, accounting for 95%, containing fluid in lemon yellow, often solitary, on one side. About 5-10% have cancerous cysts with irregular walls, thickening or calcifications, with internal echogenicity.The patient has almost no symptoms and is discovered incidentally by ultrasound, sometimes with hip pain, fever, hematuria, and increased blood pressure. To diagnose the disease, the patient will be assigned abdominal ultrasound, computed tomography to accurately diagnose and classify the risk of kidney cancer.
Endotracheal anesthesia is a technique of general anesthesia with endotracheal intubation for
purposes of respiratory control during surgery and postoperative resuscitation. This method is indicated for patients with secondary hypertension; 4cm large cyst causing discomfort to the patient; Cysts press on the excretory tract causing hydronephrosis and III IV renal cysts do not stop at cystectomy, but radical nephrectomy should be performed.
However, endotracheal anesthesia for transperitoneal endoscopic renal cyst surgery will not be performed if the patient and the patient's family do not agree to perform; The hospital does not have enough facilities for anesthesia and resuscitation. In addition, this procedure is contraindicated in the following cases:
Renal cyst type III IV according to Bosniak. Coagulopathy, serious medical disease is progressing.
Nang thận thường lành tính chiếm 95%, chứa dịch trong vàng chanh, thường đơn độc, 1 bên
2. Endotracheal anesthesia procedure for transperitoneal endoscopic renal cyst surgery
2.1 Preparation
On the hospital side: To perform endotracheal anesthesia for transperitoneal endoscopic renal cyst surgery, it is necessary to have a surgical team and a specialist anesthesiologist and nurse. At the same time, the means and tools need to be fully prepared. Specifically:Anesthesia machine system with breathing, hand-held oxygen source, vital function monitor (ECG, arterial blood pressure, SpO2, EtCO2, breathing rate, temperature) defibrillator, suction machine.. Laryngoscope, endotracheal tube of all sizes, suction tube, mask, squeeze balloon, oropharyngeal cannula, Magill pliers, soft mandrin. Lidocaine 10% spray. Salbutamol spray. Prophylaxis for difficult intubation: Cook tube, laryngeal mask, flexible bronchoscope, tracheostomy kit, mouth opener... Sleeping pills: intravenous anesthetic (propofol, etomidat) , thiopental, ketamine...), volatile anesthetics (sevoflurane...). Painkillers: fentanyl, sufentanil, morphine... Muscle relaxants (if needed): (succinylcholine, rocuronium, vecuronium...). On the side of the patient:
The patient is well explained about the disease and treatment method. Complete pre-operative tests. Pre-anesthesia examination by anesthesiologist to detect and prevent risks. Evaluation of difficult endotracheal intubation. In case the patient is anxious, the doctor may prescribe a sedative from the night before. Prepare full medical records according to regulations of the Ministry of Health, including: Commitment to surgery, pre-operative examination steps, full necessary tests...
2.2. Conduct
The patient is instructed to lie on his or her back. At the same time, 5 minutes before the induction of anesthesia, 100% oxygen should be given 3-6/min. Install monitors and establish effective transmission. Only when the patient sleeps deeply and has enough muscle relaxation can endotracheal intubation be performed. There are two techniques for endotracheal intubation: oral and nasal.2.2.1. Technique of oral endotracheal intubation
Open the mouth, put the laryngoscope and the right side of the mouth, move the tongue to the left to push the light deep. Coordinate with the right hand the thyroid cartilage lamp to find the epiglottis and glottis. Perform rapid induction of anesthesia and Sellick maneuver in case of full stomach (pressing the cricoid cartilage 20-30 kg as soon as the patient loses consciousness until the intubation is complete). Pass the endotracheal tube gently through the glottis, stopping when the balloon of the endotracheal tube passes 2-3 cm through the vocal cords. Gently withdraw the laryngoscope. Endotracheal balloon pump. Check the correct position of the endotracheal tube with auscultation and EtCO2 results. Secure the tube with tape and place the cannula in the mouth to avoid biting the tube (if necessary).
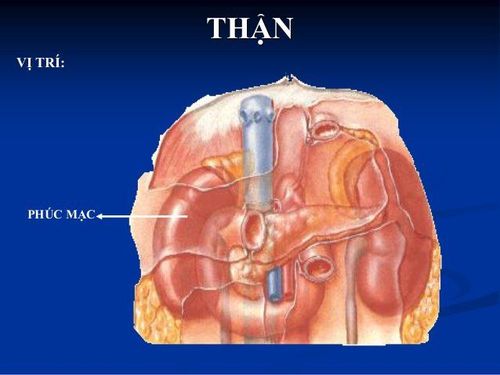
Gây mê nội khí quản phẫu thuật nội soi nang thận qua phúc mạc
2.2.2. Technique of endotracheal intubation
Choose the side of the nasal passage and drop a vasoconstrictor drug (naphazoline, otrivine...). Select an endotracheal tube size smaller than that of the oral route. Insert an endotracheal tube lubricated with lidocaine grease through the nostrils Open the mouth, insert the laryngoscope to the right side of the mouth, move the tongue to the left, push the lamp deeply, coordinate with the right hand to press the cricoid cartilage to find the rod cap. glottis and glottis. Favorable case: insert the endotracheal tube gently through the glottis, stopping when the balloon of the endotracheal tube passes through the vocal cords 2-3 cm. Use Magill pliers to guide the tip of the endotracheal tube into the correct glottis; The assistant pushes the endotracheal tube from the outside in difficult cases. Gently withdraw the laryngoscope. Endotracheal balloon pump. Check the correct position of the endotracheal tube with auscultation and EtCO2 results Fix the tube with adhesive tape. In case of difficult intubation: apply difficult intubation procedure. Maintenance of anesthesia:Maintain anesthesia with intravenous or volatile anesthetics, analgesics Muscle relaxants (if necessary). Control breathing by machine or hand squeeze.
2.3. Follow
Monitoring the depth of anesthesia based on heart rate, blood pressure, sweating, lacrimation (PRST); MAC, BIS and Entropy (if any)... Monitor vital signs: heart rate, blood pressure, SpO2, EtCO2, body temperature. Prevent the endotracheal tube from being misplaced, folded, or blocked. Follow up with a normal postoperative follow-up with monitoring of fluid coming out of the drain, if no more can be withdrawn after 24 - 48 hours and after removing the drain, if there is no more bleeding, the patient can be discharged; Cut the incision after 5-7 days.2.4. Criteria for extubation
The patient is awake, following orders. Raise the head for more than 5 seconds, TOF > 0.9 (if any). Breathe spontaneously, breathing rate within normal limits. Pulse and blood pressure are stable. Normal body temperature. There were no complications of anesthesia and surgery.3. Complications during and after endotracheal anesthesia laparoscopic transperitoneal renal cyst surgery and management
As with any surgery, endotracheal anesthesia for transperitoneal endoscopic renal cystectomy can have undesirable complications. Here are some complications that the patient may experience:Reflux of gastric juice into the airway. The patient is immediately aspirated, lying with the head low, tilting the head to the side. Simultaneously, quickly insert the endotracheal tube and clear the airway. Hemodynamic disturbances: hypotension or hypertension, cardiac arrhythmias (bradycardia, tachycardia, arrhythmia) Intubation complications Bend, retract, endotracheal tube is pushed deep into one lung, retract or open respiratory system, the source of oxygen is exhausted, soda is not effective leading to lack of oxygen. In this case, it is necessary to quickly ensure ventilation and provide 100% oxygen, find and address the cause. Respiratory failure after extubation due to many causes Sore throat hoarseness Vocal - tracheobronchospasm, upper respiratory tract inflammation... Vinmec International General Hospital is one of the hospitals that apply. strict standards of safe surgical anesthesia practice according to international guidelines. Vinmec has a team of experienced anesthesiologists and nurses, modern equipment such as: nerve detectors, ultrasound machines, Karl Storz's difficult airway control system, comprehensive anesthesia monitoring system GE's AoA (Adequate of Anesthesia) including monitoring of anesthesia, pain and muscle relaxation will provide high quality and safety, helping patients to have adequate anesthesia, not wake up, and do not have residual muscle relaxants after surgery.
Vinmec Health System is also proud to be the first hospital in Vietnam to sign with the World Anesthesiology Association (WFSA) towards the goal of becoming the safest hospital for surgical anesthesia in Southeast Asia.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
See also:Polycystic kidney disease is hereditary? Common complications of polycystic kidney Polycystic kidney: Causes, symptoms, diagnosis and treatment Anesthesia, pre-anesthesia: What you need to know