This is an automatically translated article.
The article was professionally consulted by a Doctor of Cardiology - Thoracic Surgery, Vinmec Central Park International General Hospital.Deep vein thrombosis of the lower extremities is a disease that forms when a blood clot in a vein obstructs the flow of blood back to the heart. Areas with blocked blood vessels will be painful, swollen, and bruised. If the hematoma travels to the lungs, it can cause a pulmonary embolism leading to serious breathing problems. Therefore, it is necessary to diagnose deep vein thrombosis of the lower extremities early to promptly treat the disease.
1. Diagnosis of deep vein thrombosis of the lower extremities
1.1 Definitive diagnosis Diagnosis of deep vein thrombosis of the lower extremities is based on the patient's clinical symptoms, exploitation of predisposing factors, and clinical risk assessment of DVT in order to Selection of testing and diagnostic methods.Patients with a low probability of disease will be assigned a D - dimer test. Patients with moderate or high clinical probability of disease should be indicated with intravenous Doppler ultrasound.
Clinical symptoms of deep vein thrombosis of the lower extremities include:
Pain when palpating or when flexing the instep of the foot into the lower leg; Hot foot skin ; Erythema; Increased tone; Superficial varicose veins; Reduce scabbing; Increase the circumference of calves, thighs; Ankle edema. Evaluation of clinical risk factors for deep vein thrombosis of the lower extremities according to the modified Wells score.
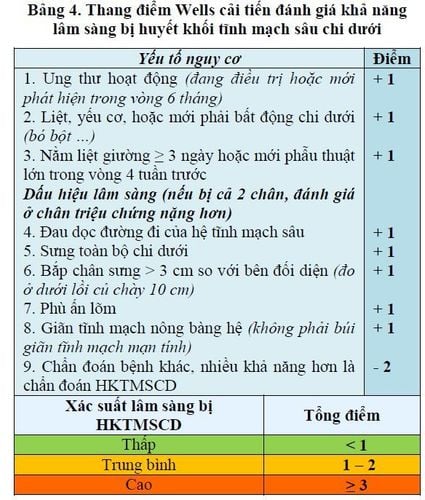
Thang điểm Wells cải tiến đánh giá khả năng lâm sàng bị huyết khối tĩnh mạch sâu chi dưới
Cellulitis: Common in patients with lower extremity venous insufficiency, lymphatic occlusion, and urinary retention. Street; Lower extremity superficial vein thrombosis: Common in patients after infusion, or patients with venous insufficiency of the lower extremities; Baker's cocoon: Symptoms of sudden swelling and pain in the calf; Intramuscular hematoma: Common after trauma, or in patients with coagulopathy (cirrhosis, overdose of anticoagulants...); Lymphatic occlusion; Drug-induced edema. 1.3. Diagnosing the cause of VTE with predisposing factors: Patients with VTE are recommended to take their medical history for a favorable risk factor for VTE.
Cases of deep vein thrombosis of the lower extremities with obvious predisposing factors, for example, patients after surgery, after trauma, cancer patients... are considered to have an underlying disease. However, about one-third of patients with deep vein thrombosis of the lower extremities are idiopathic and need to be diagnosed.
Congenital or acquired coagulation disorders: The time to do Protein C, Protein S, Antithrombine III tests is before anti-vitamin K therapy, or after stopping the use of vitamin K antagonists (stopping vitamin K antagonists). vitamin K resistance for at least 2 weeks), preferably outside of acute thrombosis (after 6 weeks).
Cancer pathology: In the case of patients with venous thromboembolism with unknown predisposing factors and never detected cancer, depending on the clinical symptoms, appropriate diagnostic tests for cancer may be indicated. Case: Clinical symptoms include: Unexplained weight loss, lymphadenopathy, hemoptysis, bloody stools, hematuria... Routine paraclinical exploration: Cardiopulmonary x-ray , abdominal ultrasound, adnexal ultrasound, vaginal smear, urine test to assess liver and kidney function, blood count test... Expanded paraclinical exploration: CT chest computed tomography , abdominal computed tomography, gastroscopy, colonoscopy, cancer marker testing.
2. Treatment of deep vein thrombosis of the lower extremities

Có thể điều trị huyết khối tĩnh mạch sâu bằng thuốc chống đông
The patient has deep vein thrombosis of the lower extremities It is recommended to treat immediately with anticoagulants; Patients with symptomatic deep vein thrombosis of the distal lower extremities (from the legs to the feet) are also recommended to receive anticoagulation immediately; The patient has asymptomatic distal acute deep vein thrombosis of the lower extremities; Patients with a high clinical probability of DVT of the lower extremities should be treated with anticoagulation as soon as the diagnosis is confirmed; Patients with a moderate clinical probability of DVT of the lower extremities should be considered for immediate anticoagulation if the waiting time for diagnostic testing is longer than 4 hours. Other treatments: Systemic (or direct catheter) thrombocytopenia should be considered in the case of acute massive thrombosis (greater than 14 days) in the iliac-femoral region, with a risk of limb necrosis. due to arterial compression, the patient's prognosis is over 1 year; Inferior vena cava filter: Indicated for patients with deep vein thrombosis of the proximal lower extremities with contraindications to anticoagulation therapy, or patients with venous thromboembolism re-embolization; Thrombectomy: Consider indication for patients with acute large iliac-femoral thrombosis, prognosis of more than 1 year, good general condition, or patients with thrombosis at risk of threatening gangrene due to compression. artery; Pressure elastic bandages, medical pressure socks: Early indication for patients with deep vein thrombosis of the lower extremities, should maintain elastic bandages for at least 2 years; Early mobilization: Patients are encouraged to mobilize early from the first day after being wrapped in elastic bandages, medical pressure socks.

Bệnh nhân được khuyến khích vận động sớm ngay từ ngày đầu tiên sau khi được quấn băng chun, tất áp lực y khoa
2.3 Treatment in the prolonged maintenance phase (3 months – prolonged) Indications for prolonged maintenance anticoagulation therapy for patients:
Predisposing risk factors, recommended anticoagulant therapy winter 3 months; Without predisposing risk factors, anticoagulation therapy is recommended for at least 3 months; Patients with first-time VTE, unknown predisposing factors, low bleeding risk, consider prolonged anticoagulation therapy; In patients with recurrent VTE, with unknown predisposing risk factors, long-term anticoagulation therapy is recommended; Patients with venous thromboembolism due to congenital causes, high thromboembolic risk, or acquired should maintain prolonged anticoagulation if the bleeding risk is low; Patients with advanced cancer, VTE and low bleeding risk are recommended to be treated with low-grade heparin TLPT for 3-6 months, then maintain long-term anticoagulation; Patients with advanced cancer, venous thromboembolism and at high risk of bleeding should maintain prolonged anticoagulation therapy. 2.4. Post-thrombotic complications Post-thrombotic syndrome is a symptom of chronic venous insufficiency secondary to lower extremity deep vein thrombosis. These symptoms include: pain, ulceration, edema, dystrophy.
Diagnosis by Doppler ultrasound, detecting reflux in the femoral and popliteal veins > 1 second; Reflux in the deep vein of the leg > 0.5 s.
Treatment:
Internal medicine: Treatment of elastic bandages or medical pressure socks in combination with rehabilitation exercises and intravenous drugs; Intervention: Place stents in the femoral and pelvic veins in case of post-thrombotic femoral - iliac vein stenosis; Surgery: Grafting or transferring deep veins, creating new deep vein valves.
Master. Doctor Nguyen Duc Hien has more than 12 years of experience in the field of cardiology, especially Cardiovascular and thoracic surgery. Currently, he is a Doctor of Cardiology Surgery, Cardiovascular Center, Vinmec Central Park International General Hospital.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.













