This is an automatically translated article.
Liver flukes are parasites that can cause disease in humans and some animals. Liver flukes cannot be passed from person to person. Instead, humans and animals become infected with liver flukes from eating contaminated fish or drinking contaminated water. So how to diagnose fascioliasis early and accurately? The following article helps you better understand the method of using anti-fasciola antibodies to diagnose fascioliasis in humans.
1. What is fascioliasis?
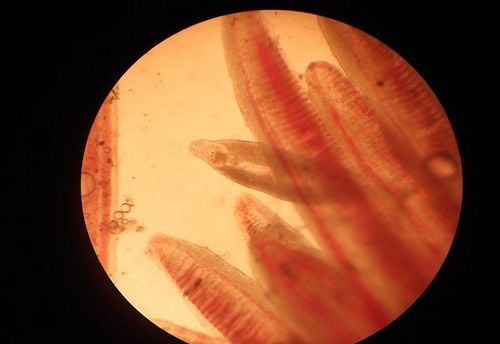
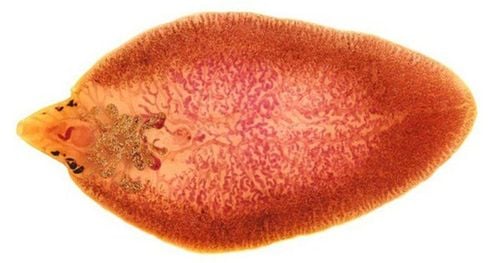
Fascioliasis (large liver fluke) is caused by the parasite Fasciola hepatica (F.hepatica) and Fasciola gigantica (F.gigantica). The disease may be caused by the passage of large numbers of immature flukes through the liver, or the presence of adult flukes in the biliary tract, or both. Liver flukes can infect all herbivores (and humans) but mainly affect sheep and cattle. It is particularly susceptible to disease in sheep.
Fascioliasis: Fasciola hepatica is distributed mainly in Europe (Portugal, UK, Turkey, Spain,); in South America (Agentina, Peru, Bolivia, Ecuador); in Africa (Egypt, Ethiopia); in Asia (Papua-New Guinea, Korea, Iran and some parts of Japan). Fasciola gigantica is distributed mainly in Asia in countries such as Taiwan, China, Japan, Korea, Philippines and Vietnam. In Vietnam up to now, fascioliasis has appeared in 47/ a total of 63 provinces and cities; The highest rate of tapeworm infection is in some provinces in the Central region and the Central Highlands such as: Binh Dinh, Quang Nam, Quang Ngai, Phu Yen, Gia Lai, Khanh Hoa, and Ho Chi Minh City. Danang.
Clinical symptoms
Invasive phase lasts 2-3 months, causing symptoms:
Fatigue, loss of appetite, weight loss May be mild fever, transient, sometimes high fever, prolonged fever The patient has feeling of fullness, dyspepsia, gastrointestinal disturbances, nausea Abdominal pain in the right lower quadrant, spreading to the back or epigastrium, can be dull, sometimes severe, sometimes no abdominal pain May be Intra-abdominal fluid, sometimes peritonitis During the invasion stage, fluke larvae can migrate out of place and cause lesions in abnormal locations such as intestinal wall, abdominal wall.
Chronic cholangitis stage: right upper quadrant pain, jaundice, liver is usually not enlarged, allergies, rash.

Giải đáp fasciola igg là gì?
2. Anti-Fasciola antibodies diagnose fascioliasis
Diagnosis of human fascioliasis is challenging. The implementation of parasitological approaches, which are based on the detection of eggs of the parasites in feces, is unsatisfactory.Current serological methods for the diagnosis of human fascioliasis are mainly based on the detection of Fasciola antibodies in serum. Although, there have been some improvements in the development of immunodiagnostic tests for the diagnosis of human fascioliasis, these tests are not sufficiently sensitive or specific.
Detection of antigens, rather than antibodies, appears to be a suitable approach in the diagnosis of human fascioliasis. Antigen can be detected in the serum or stool of patients with fascioliasis. Serum circulating antigens disappear for a short time and most circulating antigens in immunocomplex form are not available for detection.
Immunodiagnosis, based on antigen or antibody detection, are appropriate approaches for the diagnosis of human fascioliasis. This is because in human fascioliasis, the incubation period typically ranges from a few days to 2-3 months, while the prodromal period is 3-4 months or even longer.
Consequently, patients often develop clinical signs or symptoms long before eggs appear in the stool. However, Fasciola antibodies could be detected in the serum of patients two weeks after infection, suggesting that serologic tests are the appropriate technique for diagnosing infection. Furthermore, antigens can be detected in a patient's serum or stool about eight weeks after infection, again long (about two months) before ovulation begins
Multiple Antibody Detection Systems were introduced for the diagnosis of human fascioliasis, and several of these systems, including the DRG Fasciola hepatica IgG ELISA (DRG International, Inc., USA), are commercially available. One of the main advantages of the antibody detection test in fascioliasis is that antibodies can be detected almost two weeks after infection, i.e. about 2-3 months before eggs are present in the stool.
Early diagnosis and appropriate treatment of human fascioliasis can avoid tissue (liver) damage. Thus, antibody detection is a suitable method for early diagnosis and treatment of the disease.
Pseudo-infection can occur when infected animal liver is consumed shortly before sampling. Placing the patient on a liver or even meat-free diet and monitoring the patient with repeat stool testing is the primary recommended method to rule out true fascioliasis. Serological tests can also rule out these infections because these cases are serologically negative.
Existing serological antibody detection tests are unsatisfactory, because their specificity is unsatisfactory due to cross-reactivity with other helminth antigens. This is mainly due to the complexity and wide variation in immunogenicity of Fasciola antigens in both humans and animals.
Serological tests are useful for acute diagnosis, when eggs of the parasite have not yet been produced, as well as for chronic fascioliasis.
Researchers have focused on improving the ELISA system for the detection of anti-Fasciola antibodies for the diagnosis of human fascioliasis. Many antigens including crude extracts of Fasciola hepatica or Fasciola gigantica, ES antigens, purified antigens from ES or crude antigens, synthetic and recombinant antigens have been evaluated in many immunodiagnostic systems. for the diagnosis of fascioliasis in humans. Fasciola's most common antigens :
ES antigen : ES antigen is the most common source of antigens that have been used in various diagnostic tests to diagnose human fascioliasis. It is now more common to purify a component of ES and use it in diagnostic testing. Using Fasciola gigantica ES antigen, anti-Fasciola antibody was detected in 98% of fascioliasis patients in the study of Mattar MA et al. 27 KDa antigen and cathepsin are the most studied components of ES in both Fasciola hepatica and Fasciola gigantica.
Cathepsin: Cathepsin, mainly Cathepsin L1 (CL1), is the most important cysteine protease secreted by Fasciola spp. and is also the most appreciated antigen that has been widely used to develop serological tests for the diagnosis of human fascioliasis.

Mệt mỏi, chán ăn là triệu chứng của bệnh sán lá gan lớn ở giai đoạn xâm nhập
Fasciola spp (27 kDa antigen): Scientists have reported that the ES of Fasciola gigantica consists of more than six polypeptides that react with the serum of patients with fascioliasis. Among these antigens, the 27 kDa antigen was reported to be reactive with all patient serum but not with serum of healthy controls. In conjunction with this study, the antigenic components of the ES of Fasciola hepatica were evaluated by Sampaio-Silva ML et al., and the results showed that 27 kDa antigen was recognized by the sera of all diseases. large liver fluke. The 27 kDa antigen of both Fasciola hepatica and Fasciola gigantica, secreted by the parasite, appears to be an immunopredominant antigen of high diagnostic value. The antigen appears to have both N and O-glycan. It has been shown that the primary antigenicity of this antigen is due to its protein epithelium because the degraded antigen retains its antigenicity
Saposin : An indirect ELISA, using SLP 2 , was developed to detect IgG antibodies against Fasciola hepatica in human serum. Other components of ES or adult worm antigens: Proteomic approaches and immunolabeling techniques reveal that Leucine Aminopeptidase (LAP) enzymes and phosphoenolpyruvate carboxykinase are two immunopredominant antigens that react with serum of HF patients. Using two recombinant Fasciola hepatica antigens, ferritin (FhFtn_1) and a tegument-binding protein (FhTP 16-5) in the ELISA system yielded 96.6% and 91.4% sensitivity and specificity are 95.7% and 92.4%, respectively. A recombinant protein thioredoxin of Fasciola gigantica has been evaluated for the diagnosis of human fascioliasis with low sensitivity (66.7%) but high specificity (96.8%). , although considered the gold standard and differential diagnosis in some situations, is not useful for diagnosing human fascioliasis during the acute phase of the disease and because of its poor sensitivity in the early stages of the disease. chronic phase. The detection of antibodies against fascioliasis has the main advantage of being positive as early as two weeks after infection, before eggs are present in the stool. However, antibody detection tests lack sensitivity and specificity and are incapable of distinguishing between past and present infections.
Recent data provide compelling evidence that detection of coproantigen improves and simplifies the diagnosis of human fascioliasis. Antigen can be detected in the serum or stool of patients with fascioliasis. It seems that the detection of coproantigen meets the requirements expected from a reliable and non-invasive technique for the diagnosis of human fascioliasis. Although several commercial antigen detection tests are available for the diagnosis of fascioliasis in animals, there is a need to develop and improve serological tests for the diagnosis of fascioliasis in humans. much larger than animals. Promising results have been obtained with several antigen-detection-based tests for the diagnosis of human fascioliasis. serious complications, greatly affecting human health. If an infection is suspected, the patient must go to a medical facility for timely examination, testing, diagnosis and treatment.
For direct consultation, please dial HOTLINE or register online HERE. Download the exclusive MyVinmec app for faster scheduling, more convenient calendar tracking!