This is an automatically translated article.
The article was written by MSc Ho Thi Xuan Nga - Cardiac Anesthesiologist, Cardiovascular Center - Vinmec Central Park International General Hospital.Before every surgery, no matter how big or small, the doctor needs to predict the level of success, failure, the risk of possible complications for his patients. Therefore, it is always required that at least one pre-anesthesia visit be performed at least 24 hours prior to commencing surgery.
1. Death under anesthesia
In a recent French study, the mortality rate directly related to anesthesia was 0.7/100,000 procedures (1: 145,500 procedures); the mortality rate partially related to anesthesia was 4.7 per 100,000 behaviors (1:21,200).According to statistics, 12% of deaths occurred during induction of anesthesia, 26% while maintaining anesthesia and 62% upon awakening and in the postoperative period. One third of anesthesia induction accidents are caused by an overdose of anesthetics leading to hypotension and ischemia. Inadequate replacement of blood loss is responsible for 100 deaths annually in France.
An American survey during 1999-2005 gave a mean mortality rate of 0.8: 100,000 behaviors and 0.4: 100,000 of those assessed with ASA I. In this study, drug overdose and side effects from anesthetics account for 47% and 42% of deaths, respectively; Directly related mortality rates tripled over the age of 80.
In the Netherlands, the mortality rate directly related to anesthesia is 0.14: 100,000 procedures and the mortality rate related to partial anesthesia is 8.8: 100,000 procedures.
In Switzerland, the estimated anesthetic mortality from out-of-court claims varies between 0.5 and 0.8:100,000.
Cardiac anaesthesia has a high level of risk because it involves patients who are often traumatized • Brain damage: 5%.
Efforts over the past thirty years to improve safety in anesthesia have reduced the risk of death and irreversible neurological damage by 1% per year of seriousness when undergoing major surgery. This is clearly shown by the distribution of mortality associated with complete or partial anesthesia with risk group.
ASA I: 0.6: 100,000; ASA II: 5.0: 100,000; ASA III: 27: 100,000; ASA IV: 55: 100,000. In fact, a poor preoperative assessment causes about 40% of the deaths in the operating room, and 43% of these are related to inadequate coordination within the group.
Careless preparation and administration of drugs is the cause of 7% of fatal accidents. The mortality rate for difficult intubation is 12% in the operating room, but 61% in the intensive care unit.
Complications in Anesthesia While the mortality rate decreased, the complication rate remained high:
Minor complications (no sequelae or treatment): 18- 22%; Serious complications (prolonged stay, requiring treatment): 0.5-1.4%; Permanent damage (nerve sequelae, permanent hoarseness): 0.2-0.6%. The most frequent recorded damages:
Nerve damage: 40%; Airway complications: 15%; Injury during puncture of blood vessel : 7%; At the same time accidents have decreased by 30% during this period.

Tử vong trong gây mê
2. What does pre-anesthesia assessment include?
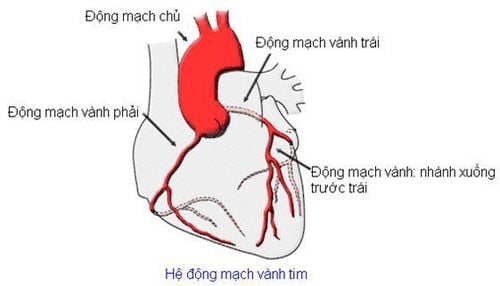
2.1 Preoperative evaluation during a cardiac surgery 2.1.1 Preoperative risk factors Several preoperatively detectable conditions are risk factors for postoperative morbidity and mortality surgery. In general, the operative mortality rate for coronary artery bypass grafting (PAC) is 0.5 to 3% depending on the risk category in elective cases and 6-8% for urgent or in multivascular patients. The mortality rate from unstable angina is 4-20%.
The risk of infarction after surgery is 2-9%. Mortality rates from simple aortic valve replacement average 2%, mitral valve replacement 3-8%, and mitral valve repair 1-4%.
In recent years, PAC mortality tends to increase by 1-2%, reflecting the fact that we operate on a higher risk population: ventricular dysfunction, diabetes diabetes, widespread coronary heart disease, advanced age.
2.1.2 Risk factors for decompensated heart failure
Patients with cardiogenic shock, with ventricular support or inotropic support (the mortality rate increases 5-7 times). Post-infarction CIV increases mortality 10-fold. The surgical mortality of PACs is directly related to left ventricular function:
EF= 0.6 mortality <1%; EF= 0.4 - 0.5 mortality 2%; EF= 0.2 - 0.4 mortality rate 4%; FE < 0.2 mortality rate 8%. Urgent surgery
Patient with unstable angina, decompensated valve disease, failed angioplasty. Surgical mortality was increased 3 times.
Renal failure
Patients with increased mortality as serum creatinine increases
Normal creatinine mortality < 2%; Creatinine > 200 mol/L mortality 8%; Creatinine > 400 μmol/L 20% mortality; Mortality on dialysis before surgery tripled. Age
Patient <65 years old, mortality <2%, neurological sequelae 1%; Patients >75 years old, mortality rate 6%, neurological sequelae 4-9%. Reoperation
The patient mortality rate is doubled, and increases with the number of surgeries.
Polyvascular condition: double mortality; Pneumonia: mortality multiplied by a factor of 1.7. Diabetes requiring insulin: mortality increases 1.5 times if blood sugar is > 15 mmol/L. Female
The increase in morbidity and mortality in female patients is largely due to the presence of more risk factors than men (cerebrovascular disease, diabetes, renal failure, obesity, hypertension). pressure and peripheral vascular disease).
Scales used to assess risk factors and predict mortality today commonly applied to open heart surgery: 2.1.3 EuroSCORE (European System of Cardiac Performance Risk Assessment) EuroSCORE allows prediction of rates intraoperative mortality after 30 days by adding the scores on the calculated scale. Use the website (www.euroscore.org/calculators.html) (www.euroscore.org/calc.html).
Age; Gender; Renal failure (3 degrees: moderate, severe, on dialysis); Peripheral artery disease Decreased mobility; History of heart surgery; COPD ; Progressive endocarditis Important preoperative state (cardiac massage, TV, inotropes, anticonvulsants, anuria); Diabetes requires insulin; NYHA grading (4 degrees: I to IV); Class IV angina; Ventricular dysfunction (4 degrees: EF > 0.5, 0.3-0.5, 0.2-0.3, <0.2); Recent infarction ; Pulmonary hypertension (2 types: PAPm 31-55 mmHg, > 55 mmHg); Urgent surgery (3 types: within 48 hours, immediate, rescue); Severity of intervention (3 types: CAP, simple surgery, combined surgery); Thoracic aortic surgery. 2.1.4 Respiratory status (COPD, asthma) The patient's respiratory status must be optimized for intervention with bronchodilators, mucolytics, physical therapy, and antibiotic therapy if necessary. It is sometimes difficult to distinguish severe symptoms of respiratory illness from pulmonary symptoms due to left ventricular stagnation (mitral disease, congestive heart failure).
Except in extreme and irreversible situations (such as vital capacity <1 L), respiratory-bronchial problems are not a contraindication to cardiac surgery, but they are an additional risk factor associated with prolonged care stay.
2.1.5 Neurological symptoms Patients with a history of stroke (stroke), transient ischemic attack (TIA), or significant carotid stenosis must undergo surgery before cardiac intervention.

Bệnh nhân có tiền sử mắc cơn thiếu máu não ngang cần được phẫu thuật trước khi can thiệp tim
2.1.6 Urinary symptoms Patients with any urinary tract infection should be treated; Prostate symptoms can make bladder catheterization difficult and necessitate the placement of a subsonic drainage.
2.1.7 Gastrointestinal bleeding The cause must be systematically examined (endoscopically) to rule out the risks of extracorporeal circulation (CEC).
2.1.8 Curing Varicose Veins The absence of large veins or varicose veins means that the possibilities of venous removal for bypass surgery of the legs or upper extremities, or the use of an arteriovenous graft, are eliminated. Any dental or ENT infection should be investigated and treated.
2.1.9 Smoking Patients who smoke should stop at least 2-3 weeks before surgery, ideally 2 months.
2.1.10 Alcoholism Look for cirrhosis, gastrointestinal bleeding and neurological disorders; Patients in child grade A are still candidates for surgical intervention, and stages B and C are generally considered contraindications to surgery.
2.1.11 Diabetes Look for complications (artery, kidney failure, etc.); The anti-diabetic diet must be continued until the day of surgery.
2.1.12 Physical Condition The physical examination of the patient should highlight a few specific points in addition to the general condition and cardiac examination.
Skin infections at surgical sites:
Cavities: any prosthetic (valve) implant requiring preoperative tooth cleaning; Ear, nose and throat condition: study and treat infection foci before valve replacement; Blood pressure difference between arms: subclavian stenosis precludes use of internal mammary artery or CEC intervention on that side; Peripheral artery disease: look for radial artery disease, femoral artery disease (arterial monitoring catheter, possibly antispasmodic), Allen test; Venous status of the extremities: looking for varicose veins in the case of venous CAP. 2.1.15 Exercise capacity Divided into 3 categories: excellent (> 9 MET), moderate (4-8 MET) or poor (< 4 MET). This stratification is a very relevant clinical estimate of the patient's functional reserve; Surgical mortality increased significantly below the threshold of 4 MET. Although this value is greater than the postoperative O2 consumption (5-7 ml O2/kg/min).
However, an individual can only maintain a cardiac output corresponding to 45% of their VO2 max for 24 hours; Therefore, 45% of the 4 METs correspond to the minimal needs of the postoperative period.
2.1.16 Carotid artery disease Carotid stenosis more than 50% is present in a quarter of patients with arterial vascular disease or coronary artery disease. Asymptomatic stenosis greater than 75% is associated with a 5% annual risk of stroke.
When there is a history of stroke, the risk of a neurological accident is 25% in the first year and 12% per year thereafter. For cardiac surgery, this risk necessitates screening of all symptomatic patients over 65 years of age.
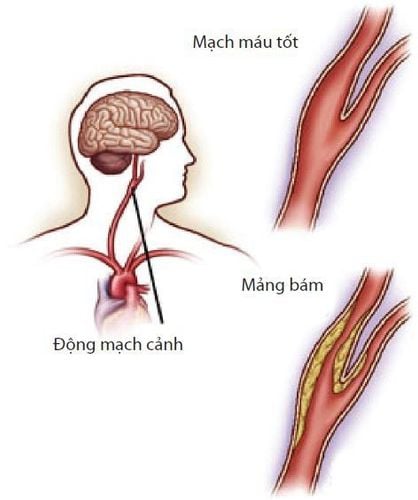
Bệnh lý động mạch cảnh
Symptomatic stenosis ≥ 60%; Asymptomatic stenosis ≥ 70%; Narrow ulcers, even <70% and asymptomatic; 100% chronic carotid occlusion is not an indication. According to the current literature, rates of coronary complications (infarction) and carotid complications (strokes) are higher in concurrent operations (7-11%) than in two-step interventions (5% ) [18]; mortality is 4-6% in the case of concurrent operations, while it is 1-2% for PACs alone and <1% for TEACs alone. The relative risk of each intervention was lower than that of the combination, which typically involves two staggered interventions: typically, TEAC is performed initially and PAC 2-4 weeks later. This delay is evidenced by the fact that cerebrovascular autoregulation is affected in 1-2 weeks after stroke or TEAC and the risk of neurological complications increases 10-fold during this period.
2.1.18 New myocardial infarction The risk of surgery is very high in the first days after the infarction. Performing surgical revascularization within 4-7 days after myocardial infarction is recommended if further damage is not desired. Urgent PAC is indicated if symptoms persist for less than 6 hours and the infarct area is at great risk. The risk of bleeding is very high in patients who have received thrombolytics in the previous 12 hours or who are taking high doses of antiplatelet agents. In hemodynamically unstable cases, preoperative intra-aortic balloon counterpulsation maintains coronary perfusion.
2.1.19 Threat of Infarction Patients with unstable angina and threatened infarction often receive continuous infusions of nitroglycerin and heparin, as well as high-dose antiplatelet therapy, pending short-term PACs. . Regardless of the hemodynamic instability that occurs, the mandatory nitro infusion must be continued until revascularization activity resumes. The heparin infusion was continued until the surgical cannula was reached. Since the risk of intraoperative bleeding is still greater than usual, an adequate supply of fresh blood bags and coagulation products should be provided.
2.1.20 Cardiac Examination and Tests Required for a Cardiac Surgery Common laboratory tests required for cardiac surgery are:
Complete blood count, TP, PTT, thrombosis, fibrinogen ; Na +, K +, Mg 2+, Ca 2+, urea, creatinine, blood sugar, protein (albumin); CK-MB, troponin if recent infarction; Total urinalysis; Look for hidden blood in the stool; Blood group; Cross-reactivity test (usually order 4 red blood cells concentrate); Measure arterial blood gas in case of cyanosis; Chest X-ray straight and inclined; ECG ; Transthoracic echocardiography ; Pulmonary function measurement (optional): Stress test (optional); Cardiac catheterization and coronary angiography (if indicated); Medical examination and dental examination; Throat smear; Echocardiography : has become effective enough to provide all the necessary data for surgical indications; Interventional cardiac catheterization: only done in suspected cases. Coronary angiography: if male patient is over 45 years old and female patient is over 50 years old, or in case of ischemic symptoms. Vinmec International General Hospital is one of the hospitals that not only ensures professional quality with a team of leading doctors, modern equipment and technology, but also stands out for its examination and consulting services. and comprehensive, professional medical treatment; civilized, polite, safe and sterile medical examination and treatment space. Customers when choosing to perform tests here can be completely assured of the accuracy of test results.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.