This is an automatically translated article.
Article by Master, Doctor Mai Vien Phuong - Gastrointestinal endoscopist - Department of Medical Examination & Internal Medicine - Vinmec Central Park International General Hospital.
The classification and diagnosis of pancreatic cystic lesions is an important issue in planning further management. Endoscopic ultrasound and transcapillary diagnosis are the two main endoscopic methods used. EUS-guided fine-needle aspiration (FNA) cytology and microneedle biopsy... are promising methods that have been used in differential diagnosis.
1. Pancreatic cystic lesions (PCL) on the rise
Currently, pancreatic cystic lesions (PCL) are commonly reported with increasing frequency and become a more common finding in clinical practice. Their detection rates are increasing with advances in imaging technology, and the detection rate of unsuspected small pancreatic cystic lesions is increasing. The frequency of detection of pancreatic cysts reported in the literature ranges from 0.7% to 36.7%. They cover a broad spectrum of entities ranging from benign cysts to malignant or malignant cystic lesions. They vary widely in clinical presentation and malignancy making these lesions diagnostically challenging.
The classification and diagnosis of pancreatic cystic lesions is considered an important issue for planning subsequent management. Endoscopic ultrasonography (EUS) and transcapillary diagnosis are the two main endoscopic methods used. EUS-guided fine-needle aspiration (FNA) cytology, EUS-guided fine-needle confocal laser endoscopy (nCLE), and microneedle biopsies are promising methods that have been used. in the differential diagnosis of mucinous and non-mucinous pancreatic cysts.
2. Benefits of EUS Method and Biopsy via EUS This is a major challenge because many benign and malignant cystic lesions as well as inflammatory cysts have a similar endothelial appearance. Furthermore, enabling assessment of cysts by EUS-FNA for early diagnosis or prognosis is a major concern to increase diagnostic accuracy for more appropriate management. EUS-FNA allows the use of aspirated samples for cytological examination and biochemical analysis, providing the opportunity to further enhance medical diagnosis and decision-making. Therefore, the addition of FNA to different imaging modalities is associated with increased diagnostic accuracy of pancreatic cystic lesions.

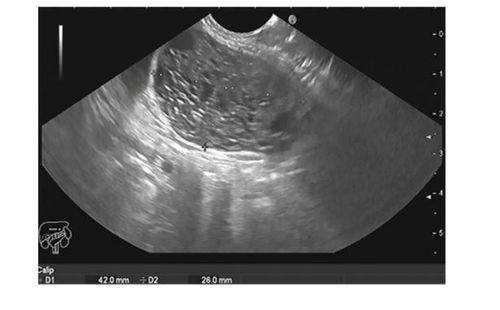
Nội soi hút kim nhỏ có hướng dẫn siêu âm của một khối u nang tuyến tụy.
The combination of both EUS-FNA links with cyst tumor marker analysis, along with clinical, radiological, histological, genetic and molecular features, improves the diagnostic accuracy of the lesion. pancreatic cystic lesions and help build a new model in the age of diagnosis of pancreatic cystic lesions. EUS-guided radiofrequency ablation (EUS-RFA) is currently considered an alternative to performing major surgery with high morbidity and mortality for small, primary pancreatic lesions. Weakness is benign. Thanks to the EUS probe's close contact with the liver, from the transgastric and transduodenal glands, the EUS allows a good visualization of the liver anatomy and its vascular system by providing detailed images, which plays an important role in detecting small-sized liver metastases from malignant pancreatic lesions, as well as potentially obtaining EUS-FNA with higher diagnostic accuracy. This can be achieved in most liver segments except for segments VII and VI, which are difficult to see on EUS examination.
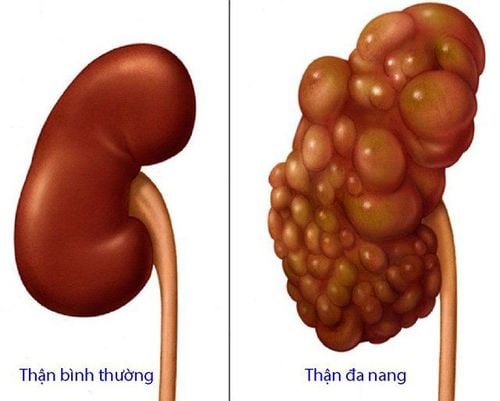
3. Classification and diagnosis of pancreatic cystic lesions Pancreatic cysts are classified into inflammatory fluid and cancerous or noncancerous pancreatic cysts. They may also be associated with other diseases such as polycystic kidney or Von Hippel Lindau.
According to the revised Atlanta classification, cases of inflammatory exudate are further classified into acute peripancreatic fluid, pseudocyst, acute necrosis, and septal pancreatitis.
Pancreatic cysts can range from simple to complex cysts, so proper diagnosis and management are important. For example, mucinous cysts carry potentially unpredictable malignant changes. Different methods are used to diagnose the type of cystic lesion such as ultrasound imaging, cytological examination of the cyst fluid, and analysis of tumor markers from the cyst fluid.
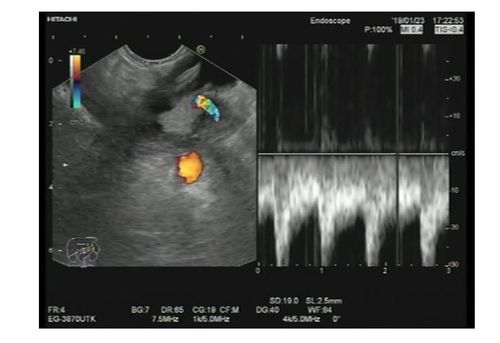
Khối u nang nhầy ở đuôi tụy với nốt hình vẽ cho thấy một mạch máu bên trong.
U nang tuyến huyết thanh vi mô của thân tụy.
| Loại u nang | CEA | CA-19-9 | Amylase | Nhuộm Mucin |
| Nang giả viêm | Bình thường | Bình thường | Bình thường | Âm tính |
| U nang bạch huyết | Bình thường | Bình thường | Bình thường | Âm tính |
| U nang tuyến tính | Bình thường | Bình thường | Bình thường | Âm tính |
| U nang nhầy | ↑ | ↑ | Bình thường | Dương tính |
| U nhầy nhú trong ống tuỵ | ↑ / Bình thường | ↑ / Bình thường | ↑ / Bình thường | Dương tính |
| U nhú đặc | - | - | - | Âm tính |
The real clinical challenge in the management of pancreatic cystic lesions is to determine which patients should undergo pancreatectomy because of early non-metastatic cancer and high-risk precancerous cystic lesions during appropriate observation. in patients with limited or no potential for malignancy. In the context of the many facets of EUS management of pancreatic cystic lesions, the currently available data are insufficient to make evidence-based decisions.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
References:
Okasha HH, Awad A, El-meligui A, Ezzat R, Aboubakr A, AbouElenin S, El-Husseiny R, Alzamzamy A. Cystic pancreatic lesions, the endless dilemma. World J Gastroenterol 2021; 27(21): 2664-2680 [DOI: 10.3748/wjg.v27.i21.2664]