This is an automatically translated article.
The article was written by Doctor Mai Vien Phuong - Department of Examination & Internal Medicine - Vinmec Central Park International General HospitalColonic diverticulum is a common disease in the elderly, often without symptoms, unless these diverticula become inflamed, also known as diverticulitis.
1. What is a colonic diverticulum?
Diverticula are small, bulging pouches that can form anywhere in the digestive tract, from the esophagus to the stomach, small intestine, and large intestine. However, they are usually found in the large intestine. Diverticulosis is a fairly common disease, often seen in patients over 40 years of age.When there is a diverticulum in the digestive system, the condition is called diverticulosis. Patients may never know they exist in the body because they rarely cause any problems, unless the diverticula become inflamed.
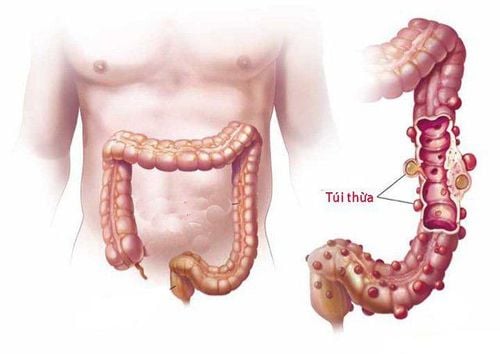
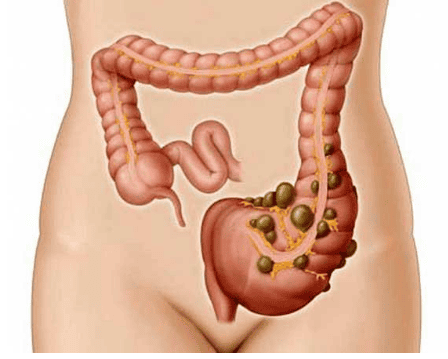
Colonic diverticula are pouch-like structures that develop in the wall of the colon, most commonly in the sigmoid and left colon, but can also involve the entire colon. When these diverticula become infected, it causes diverticulitis.
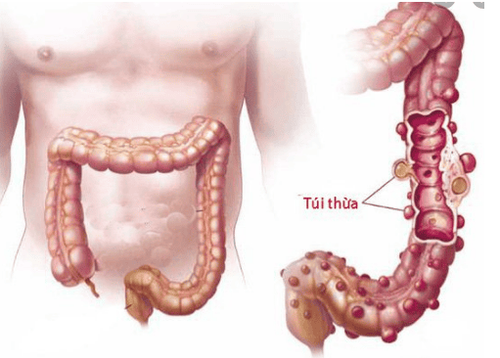
Hình 1: Bệnh lý túi thừa đại tràng
2. Diagnosing colonic diverticulitis
Based on history and physical examination (pain in the left iliac fossa); blood test to detect white blood cell count - a sign of an infection; X-ray of the colon : Determine the extent of the disease; CT scan: Differentiate inflammatory or infected diverticulum; Flexible anorectal endoscopy: View of the inside of the colon, providing additional information for diagnosis and treatment. Vinmec International General Hospital is one of the hospitals that not only ensures professional quality with a team of leading medical professionals, a system of modern equipment and technology. The hospital provides comprehensive and professional medical examination, consultation and treatment services, with a civilized, polite, safe and sterile medical examination and treatment space. Customers when choosing to perform tests here can be completely assured of the accuracy of test results.

Bệnh viện Đa khoa Quốc tế Vinmec có đầy đủ các dịch vụ khám chữa bệnh
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
3. Treatment of diverticulitis of the colon
Treatment of diverticulitis is mainly to treat infection, rest the colon and minimize complications. Specifically:
a, With mild diverticulitis, without complications
Outpatient treatment with antibiotics, analgesics and antispasmodics as prescribed by the doctor; Rest the colon by fasting or eating sparingly for a few days, then eating liquid, high-fiber foods (whole grains, fruits, and vegetables) until the pain is gone. With severe diverticulitis, frequently recurring b, If diverticulitis is severe, the pain is severe, the patient needs to be treated as an inpatient at the hospital:
Infusion of fluids, antibiotics into the vein and monitoring progress , complications of the disease; If the disease does not improve after 3 days of taking antibiotics, has enteritis, has pus pocket, peritonitis, it is necessary to surgically remove the part of the colon with the inflamed diverticulum. There are two types of surgery: one-stage bowel resection and two-stage bowel resection + colostomy. With a single-stage bowel resection, the doctor cuts off the portion of the bowel that contains the diverticulum, and then reconnects the uninflamed segments of the large intestine, allowing normal bowel movements. And 2-stage enterectomy and stoma are indicated for patients with severe colitis, the doctor could not connect the colon and rectum in the first surgery. During surgery, the doctor will open a hole in the abdominal wall, connecting the large intestine into it to remove waste. After a few months, when the inflammation has healed, the doctor will perform a second surgery to reattach the cut intestine.
4. Surgical treatment in diverticulitis of the colon
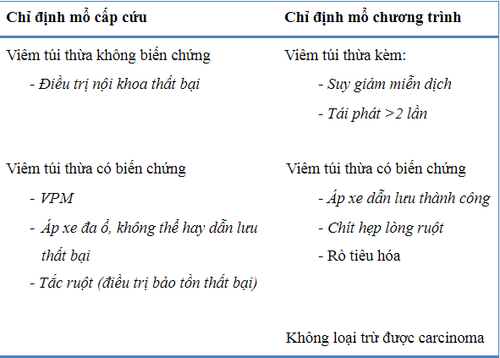
Bảng 1. Chỉ định mổ trong VTTĐT
The overall rate of CRC requiring surgical intervention is about 10-20%. Indications for surgery are mostly in subgroups II and III according to the European Society of Laparoscopic Surgery and in grades III and IV according to Hinchey. Only a small percentage of CRCs that simply require surgery are patients who do not respond to medical therapy (no improvement or worsening symptoms) after 3 days of treatment.
The goal of surgery is to resolve the infection (diverticulectomy, colectomy, drainage of the abscess, abdominal lavage...), treatment of associated complications such as intestinal obstruction, gastrointestinal fistula, and recovery. intestinal circulation with the lowest morbidity and mortality.
The surgical method can be performed in one stroke or two stages with different variations depending on the emergency surgery or program and the severity of the disease. Preoperative preparation is also very important. If emergency surgery is not required, the patient should be prepared for the colon, using antibiotics to reduce the rate of surgical site infection.
The patient should be informed of the possibility of a colostomy and the placement of the colostomy should also be taken into account for the best convenience of the patient. For Hartmann surgery, patients should also be warned that the possibility of closing the colostomy is only 60%.
For emergency surgery, open surgery with a midline incision is an appropriate option. Evaluation of criteria such as intra-abdominal infection status, degree and location of bowel obstruction, and amount of stool remaining in the colon during surgery help determine the possibility of performing an anastomosis right in surgery.
References:
Le Huy Luu, Nguyen Van Hai (2010), "Results of right colonic diverticulum surgery by laparoscopic surgery", Medicine of Ho Chi Minh City, volume 14 (additional copy of No. 4), p.12-15. Ly Minh Tung, Nguyen Van Hai (2011), Clinical features, images, and surgical results for diverticulitis. Aldoori W.H., Giovannucci E.L., Rockett H.R., et al. (1998), "A prospective study of dietary fiber types and symptomatic diverticular disease in men", J Nutr, Vol.128 (4), p.714-719. Ambrosetti P., Robert J.H., Witzig J.A., et al. (1994), "Acute left colonic diverticulitis: a prospective analysis of 226 consecutive cases", Surgery, Vol.115 (5), p.546-550.