This is an automatically translated article.
Posted by Master, Doctor Mai Vien Phuong - Department of Examination & Internal Medicine - Vinmec Central Park International General Hospital
In the Correa gastric carcinogenesis model, Helicobacter pylori infection, atrophic gastritis, and intestinal metaplasia were associated with gastric cancer development. Low serum levels of pepsinogens are known to be strongly associated with extensive atrophic gastritis. High resolution and magnified narrow band imaging (M-NBI) provides detailed examination of the gastrointestinal mucosa. However, there are no comparative data on the usefulness of standard endoscopy and M-NBI for H. pylori infection and gastric precancerous conditions.
The authors found a significant association between endoscopic mucosal patterns and the severity of gastric precancerous conditions (moderate to severe atrophic gastritis and serum pepsinogen I/II ratio ≤3). . These results appear to be valuable for identifying an at-risk group for gastric cancer by high-quality endoscopy.
1. Update on the association between Helicobacter pylori infection and gastritis
The global prevalence of Helicobacter pylori (H. pylori) infection is reported to be > 50%. In stomachs infected with H. pylori, chronic active inflammation of the mucosa becomes persistent, leading to atrophic gastritis and intestinal metaplasia (intestinal metaplasia). According to Correa's gastric carcinogenesis model, atrophic gastritis and intestinal metaplasia are associated with gastric cancer progression. Progressive gastric atrophy and intestinal metaplasia are considered precancerous conditions because they correlate with gastric carcinogenesis. Accurate diagnosis of gastric precancerous conditions is essential to identify patients at risk for gastric cancer.
2. Role of magnified NBI and NBI image modes
Narrow band imaging (NBI) is an innovative optical method for detailed examination of the gastric mucosa. Furthermore, magnified NBI endoscopy (M-NBI) with 80x magnification can visualize the smooth mucosal structures and microvessels. M-NBI endoscopy can be used to diagnose H. pylori infection and to classify gastritis according to histological grade. Recent improvements in the resolution (>1 million pixels) of gastrointestinal endoscopy have enhanced the image quality, facilitating the characterization of gastric mucosal tissue. Close observation of the gastric mucosa by standard endoscopy without magnification allows the prediction of H. pylori gastritis. Furthermore, the severity of atrophic gastritis and intestinal metaplasia varied according to endoscopic mucosal morphology. In a systematic review, standard endoscopy was effective as an alternative for the diagnosis of H. pylori infection. However, there are no comparative data on the utility of standard endoscopy and M-NBI for the diagnosis of H. pylori infection, atrophic gastritis, and intestinal metaplasia.
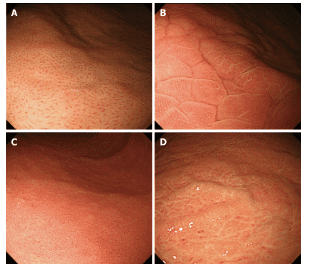
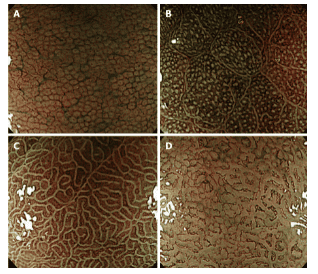
Micromucosal morphologies in the gastric body are observed with magnified narrow-band endoscopic imaging. A: The normal pattern is characterized by a regular arrangement of collecting venules and a honeycomb-like subepithelial network of capillaries; B: Type Z-1, regular round pits with polygonal grooves; C: Type Z-2, more linear and dilated pits without sulci; D: Type Z-3, loss of gastric fossa with coiled microtubules.
3. Histopathological assessment plays an important role in endoscopic diagnosis of gastrointestinal diseases.
Endoscopists tend to focus on detecting abnormal lesions, and conventional endoscopic macroscopic examination has limitations in characterizing mucosal lesions. Therefore, the final diagnosis of detected lesions is dependent on the pathology report. To identify individuals at risk for gastric cancer, the presence of precancerous conditions was assessed by protocol-specific non-targeted biopsies in different areas. However, multiple mucosal biopsies increase medical costs and procedure time.
4. Endoscopy with high resolution and high magnification facilitates detailed examination of the gastrointestinal mucosa.
In 2002, Yagi et al. used magnifying endoscopy to show that RAC was a characteristic finding in a normal stomach without H. pylori infection. Abnormal mucosal patterns without RAC are classified from Z-1 to Z-3 according to the extent of mucosal damage in the stomach infected with H. pylori. Anagnostopoulos et al demonstrated that magnified endoscopic examination could identify normal gastric mucosa, H. pylori–Associated gastritis, and atrophic gastritis in Westerners. The severity of chronic gastritis was investigated based on the micromucosa patterns observed by M-NBI. Kanzaki et al. reported that the grooved mucosa had a higher degree of intestinal atrophy and metaplasia than the follicular mucosa. However, M-NBI endoscopes are not available in all endoscopy units and training is required prior to clinical application.
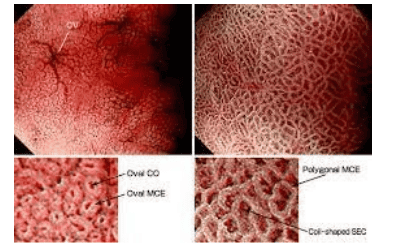
Hình ảnh niêm mạc dạ dày trên nội soi phóng đại có chức năng nhuộm màu điện tử NBI
5. Evaluation of H. pylori infection by high resolution endoscopy
In a previous study, the authors determined H. pylori infection by closely observing the gastric mucosa with high-resolution endoscopy without magnification. The sensitivity and specificity of all abnormal samples for predicting H. pylori infection were 93.3% and 89.1%, respectively, and the overall diagnostic accuracy was 91.6%. Observer and internal agreement for endoscopic mucosal patterns was 91.7% and 90.0%, respectively. This simplified endoscopic technique has allowed reliable prediction of gastric H. pylori infection in other countries. Recent advances in endoscopic imaging technology have increased the diagnostic accuracy of H. pylori infection. To the authors' knowledge, this is the first study to compare the diagnostic performance between standard endoscopy and M-NBI endoscopy for H. pylori infection. The authors also analyzed the extent of atrophic gastritis, intestinal metaplasia and serum PG levels according to two endoscopic classifications. A decrease in the serum PG I/II ratio is thought to be a noninvasive marker for advanced gastritis and gastric cancer.
6. Serum Pepsinogen is strongly correlated with gastric intestinal metaplasia and gastric cancer
Wang et al. reported that serum PG levels were strongly correlated with the OLGA gastritis classification and the OLGIM intestinal metaplasia staging classification. Therefore, a serum PG I/II ratio ≤3 is a serological marker of gastric precancerous conditions. Except for the sensitivity, the diagnostic efficacy of H. pylori infection was similar between standard endoscopy and M-NBI endoscopy. Seven patients with normal appearance by standard endoscopy were infected with H. pylori . In contrast, these patients were classified as type Z-1 (n=4), type Z-2 (n=2) and type Z-3 (n=1) by M-NBI endoscopy. This may be due to the ability of the M-NBI to examine the superficial microscopic morphology of the gastric region and fossa tissue, which is not possible with standard endoscopy. However, standard endoscopy may allow the detection of H. pylori infection in routine clinical practice (diagnostic accuracy, 93.3%).
7. Progression of atrophic inflammation of the gastric mucosa
For the diagnosis of atrophic gastritis and intestinal metaplasia, standard endoscopy and M-NBI have excellent sensitivity, NPV values (> 95%) and AUC (> 0.7); however, specificity and PPV values were not accepted.
According to the Kimura-Takemoto classification, atrophic gastritis develops more often along the lesser curvature than the great curvature of the body. As the atrophic change extends to the anterior and posterior mucosa of the body, the pattern of intestinal metaplasia becomes more diffuse in the stomach. In this study, the authors focused on the mucosal model at the greater curvature of the gastric body. Gastric mucosal atrophy and transformation to intestinal metaplasia occur ultimately at the greater curvature of the body, hindering the assessment of gastric precancerous conditions. A systematic screening procedure for the stomach has been developed to ensure high-quality endoscopic evaluation, and to allow the detection of atrophic gastritis and intestinal metaplasia in different regions of the stomach.
Using the NBI without magnification, Pimentel-Nunes et al created an endoscopic classification to classify gastrointestinal metaplasia; a tubulovillous mucosal model that is highly consistent with histological intestinal metaplasia. However, the results of enhanced endoscopy for the diagnosis and classification of atrophic gastritis are still to be established.
8. Histological picture of gastritis caused by H.Pylori . infection
Infection with H.Pylori bacteria often causes congestive edema in the gastric mucosa and antrum. Histologically, H. pylori infection causes infiltration of neutrophils and monocytes in the gastric mucosa. In biopsies, lymphatic hyperplasia is a specific immune response to H. pylori infection. During long-term H. pylori-induced inflammation, the presence of lymphatic hyperplasia decreased as the severity of atrophic gastritis and intestinal metaplasia increased. In young women, nodular gastritis due to H. pylori infection and lymphoid cysts in the nodular lesion can be detected histologically.
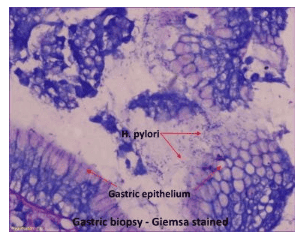
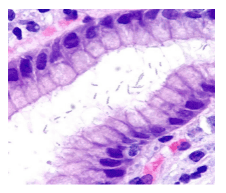
Hình ảnh xoắn khuẩn H.Pylori được nhìn thấy dưới kính hiển vi
Conclusion
In conclusion, close observation of gastric mucosa by standard endoscopy and M-NBI allows the diagnosis of H. pylori infection and gastric precancerous conditions. Furthermore, the authors' results showed an association between endoscopic mucosal patterns with moderate to severe atrophy and a serum PG I/II ratio ≤ 3.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.