This is an automatically translated article.
The article is professionally consulted by Doctor Vo Thi Thuy Trang, Department of Medical Examination & Internal Medicine - Vinmec International Hospital Da Nang.Currently, the causes of alcoholism and smoking are more common than the causes of mechanical obstruction in acute pancreatitis. The most common types of acute pancreatitis are acute edematous pancreatitis and acute necrotizing pancreatitis. If the disease is not diagnosed and treated promptly, it can lead to many dangerous complications or even death.
1. What is acute pancreatitis?
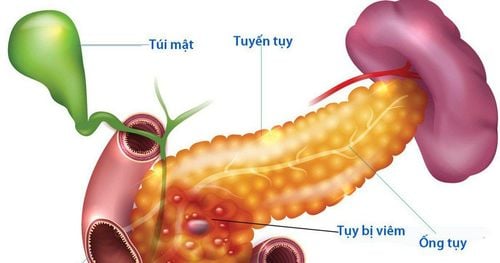
Acute pancreatitis is an acute inflammation of the pancreas leading to follicular cell damage due to the destruction of pancreatic enzymes, ranging from mild to severe and can lead to many complications, even death.People who often suffer from acute pancreatitis can be:
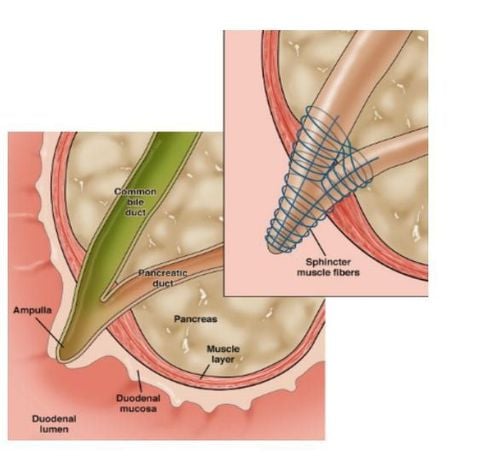
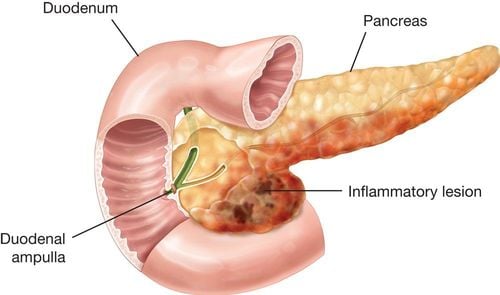
Alcoholism, smoking: now this cause is more common than mechanical obstruction. Obstruction: common bile duct stones, pancreatic tumors or ampulla of Vater, worms in the bile ducts or foreign bodies... After surgery in the peripancreatic area, after endoscopic cholecystectomy - retrograde pancreas. Due to blunt trauma to the pancreas. Due to metabolic disorders such as: hypertriglyceridemia, hypercalcemia. People with a family history of pancreatitis; Other causes such as infections, parasites, viruses, stomach ulcer drugs... About 10-15% of cases, no cause can be found. Acute pancreatitis in children is often related to many medical conditions. different reasons. If not diagnosed and treated in time, acute pancreatitis can progress to pancreatic necrosis, usually pancreatic necrosis is rarely localized but spreads due to pancreatic lysis under the influence of proteolytic enzymes. and lipids are activated in the lumen of the pancreas. This will then lead to pancreatic bleeding, even necrosis of the surrounding organs such as necrosis of the mesenteric vessels causing intra-abdominal bleeding, perforation of the duodenum, colon... later it will become an abscess. pancreas. The patient died from bleeding and septic shock.
Mortality from acute pancreatitis can reach more than 15% and death in acute alcoholic pancreatitis is 3 times higher than in acute pancreatitis due to stones or worms.
2. Possible types of acute pancreatitis
Acute pancreatitis with edema: Pancreatic edema is pale or gray, edema spreads to surrounding tissues, leaves and retroperitoneal space, and there is clear fluid in the abdomen.Acute necrotizing pancreatitis: The pancreas is enlarged irregularly with gray or dark gray necrotic foci, mixed with dark red bleeding, localized in part or all of the pancreas. Intra-abdominal fluid is dark red with blood, sometimes cloudy around the pancreas or many areas of the abdomen. Fat necrosis manifests as ivory-white candle spots on the surface of the pancreas, omentum, or throughout the abdomen.
3. Symptoms of acute pancreatitis

Triệu chứng nôn, buồn nôn thường xảy ra sau đau, nôn xong không đỡ hay hết đau
3.1. Symptoms Abdominal pain: sudden onset usually after a delicious meal and alcohol. pain is often prolonged and severe, concentrated in the epigastric region, spreading to the back or to the chest Vomiting, nausea: usually occurs after pain, vomiting does not improve or go away (other than acute gastritis), often vomiting gastric juice, bile, severe cases may vomit dilute blood. Loose stools are sometimes present. 3.2. Physical symptoms Abdominal distention and defecation: Most common with severe forms of acute pancreatitis, in some cases, frequent loose bowel movements. Reaction or spasticity of the abdominal wall due to pancreatic juice causes peritonitis, in addition to edema and hemorrhage in the abdominal cavity and retroperitoneum. Jaundice is seen in patients with biliary tract disease, especially common bile duct stones. Low back pain; Low-grade percussion In the late stages, a soft mass of indistinct border may be palpable in the epigastrium, usually due to accumulation of pancreatic juice in the omentum harem. 3.3. Systemic symptoms Whole body in toxic state, pale skin, small rapid pulse, low blood pressure showing shock, moderate or high fever. Disorders of respiratory, circulatory and urinary functions, especially in acute pancreatitis with multi-organ failure 3.4. Subclinical ● Blood Amylase: Usually increases 4 to 12 hours after pain, in edematous acute pancreatitis Amylase usually decreases after 3 to 4 days, in acute pancreatitis, it must be increased more than 3 times normal.
● Urinary amylase: Amylase is absorbed and eliminated in the urine, so it usually increases more slowly after 2 - 3 days, usually peaks on day 4 - 5 and lasts 5-7 days.
● Blood Lipase: Usually increased in parallel with blood Amylase but more specific.
● Blood sugar: Initially due to the release of Glucagon, blood sugar may be increased or due to necrosis of the islets of Langerhans, blood sugar may be greater than 11 mmol/l. High blood sugar has a severe prognosis.
● Blood calcium: There is a decrease in severe acute pancreatitis, usually appearing on days 2 - 3 and lasting for a few weeks, blood calcium < 2mmol/l is a severe prognosis.
● LDH: Increased in acute necrotizing pancreatitis when LDH > 350Ul/l means a severe prognosis.
● Arterial blood gas: Acidosis in severe cases.
● Blood count: High neutrophils, especially acute pancreatitis caused by worms and stones, when white blood cell count >16000/mm3 is a serious factor.
● Pancreatic ultrasound: The pancreas is large, the structure is poorer than normal, ultrasound also helps to detect intra-abdominal fluid, worms, stones or its complications such as abscesses and pancreatic pseudocysts.
Density computed tomography (CT Scanner): has 5 stages: A (No abnormality detected), B (Focused or diffuse large pancreas), C (Mild inflammation around the pancreas), D (Local fluid collection) residence). E (Condensation in at least 2 areas). Has prognostic significance.
● X-ray: often of little value in diagnosing acute pancreatitis, in the case of multiple bowel paralysis, there may be an image of the bowel loop.
4. Treatment of acute pancreatitis
General principles: Active medical treatment, close monitoring to have indications for timely surgical intervention.4.1 Conservative treatment The first stage of acute pancreatitis is edematous acute pancreatitis, medical treatment at this stage is largely successful, even if acute pancreatitis edematous with mild bleeding can also be cured without surgery. Conservative treatment includes:
● Decreased pancreatic secretion: by (1) Inserting a nasogastric tube for continuous aspiration of gastric juice in severe acute pancreatitis or with gas and vomiting. (2) Anti-secretory drugs such as H2 receptor blocker (AntiH2), intravenous proton pump inhibitor (IPP) have an indirect effect on reducing pancreatic secretion. (3) Somatostatin, Octreotide 100mcg
Pain relief. Anti-infective. ● Resuscitation against shock, circulatory, respiratory, endocrine, electrolyte and other systemic disorders. Too high of triglycerides can lead to plasma filtration. Kidney failure: dialysis...
Fasting, parenteral nutrition. ● Antibiotics: Mild acute pancreatitis is not indicated for antibiotic use, severe acute pancreatitis, especially acute necrotizing pancreatitis with risk of infection, is indicated for antibiotics, so choose antibiotics that penetrate the pancreas well such as: metronidazole, quinolones, 3rd generation cephalosporins, imipenem.
Closely monitor the progress of the disease to switch to emergency surgery when indicated. 4.2. Treatment according to the cause Acute stone pancreatitis: ERCP conducts early stone removal, surgery if ERCP fails.
Case of acute pancreatitis caused by worms entering the common bile duct for patients with early deworming by Fugacar, Zentel, ...
4.3. Surgical intervention Surgery is required in the following cases:
The disease is gradually getting worse with threatening signs of pancreatic necrosis: The disease is gradually getting worse with threatening signs of pancreatic tissue necrosis. :
Increased intoxication; Pain does not decrease, abdominal muscle reactivity increases. Blood and urine amylase tests did not decrease or even increased despite aggressive medical treatment. It is possible that blood and urine amynaza decreased, but the toxicity increased, the reaction of the abdominal wall increased, which is a bad sign, showing that the pancreatic cells are severely necrotic with a large area. Acute pancreatitis due to biliary tract disease: biliary obstruction with acute pancreatitis. There is doubt in the diagnosis:
Suspected gastroduodenal perforation Suspicion of necrotizing cholecystitis Suspicion of intestinal obstruction (exploratory surgery). Complicated acute pancreatitis:
Hemorrhagic necrosis Pancreatic abscess The degree of surgery depends on the specific injury of each patient and is decided by the surgeon:
After laparotomy, clean up all secretions . Open into the omentum omentum to probe the lesion. Management of specific pancreatic lesions: Drainage of the pancreas and abdomen; do adjuvant surgery if deemed necessary; check, clean the abdominal cavity, close the abdomen. If edematous acute pancreatitis without necrosis: Release the pancreas with Novocaine 0.25%; Opening the pancreatic capsule when the edema is much helps reduce pressure and improve tissue circulation, preventing necrosis. Acute necrotizing pancreatitis : Enlarge the pancreatic capsule to check; remove necrosis; careful hemostasis; release pancreatic blockage; pancreatic and abdominal drainage; drain the gallbladder or common bile duct. If there is necrosis of the body and tail of the pancreas: the body and tail of the pancreas must be removed together with splenectomy, sometimes the whole pancreas must be removed if the necrosis is complete, but it is difficult to do because the patient's condition does not allow and only drainage. pancreas, insert sesame mask to strengthen, clean and drain the abdomen.
5. Prevention of acute pancreatitis

Uống rượu có trách nhiệm hoặc không uống rượu để phòng ngừa viêm tụy cấp
Acute pancreatitis is also often caused by gallstones, so to prevent gallstones, you need to choose a healthy diet, lots of fresh fruits and vegetables every day.
Maintain a healthy weight by eating less fat: eat less fat by eating more whole-grain bread, oats and brown rice to reduce cholesterol in your body. At the same time, every day you should set aside 15 to 30 minutes for exercise, reducing the risk of developing this disease.
Periodic deworming.
Specialist Doctor I Vo Thi Thuy Trang is trained in gastroenterology, hepatobiliary tract and gastrointestinal endoscopy; continuously updated and received advanced endoscopic training from professors and endoscopy experts from Switzerland and Japan; participated in many domestic and international gastroenterology and endoscopy conferences.
With nearly 20 years of working at Da Nang General Hospital in the field of gastrointestinal endoscopy - hepatobiliary disease, every year, Doctor Vo Thi Thuy Trang participates in endoscopy more than 1500 cases including: endoscopic diagnosis of diseases stomach, colon such as: detecting inflammation, ulcers, polyps, cancer, finding HP bacteria, detecting cancer early in the digestive tract...; Endoscopic treatment such as: Hemostasis in gastrointestinal bleeding, esophageal varices ligation in cirrhosis, endoscopic gastrointestinal polypectomy...
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.