This is an automatically translated article.
The article is professionally consulted by Master, Doctor Vu Huy Binh - Department of Medical Examination & Internal Medicine - Vinmec Hai Phong International General Hospital.Small bowel obstruction is a partial or complete blockage of the small intestine. Small bowel obstruction can be caused by many causes such as adhesions, hernias and inflammatory bowel disorders, etc. Current treatment methods for small bowel obstruction include medical treatment and surgery.
1. What is small bowel obstruction?
Intestinal obstruction is the interruption of intestinal circulation, which can be blocked in one or more locations, from the pylorus to the anal canal, leading to vomiting (possibly vomiting of bile) and abdominal pain.People with small bowel obstruction are mostly caused by sticky cords. Most adhesions that cause bowel obstruction are pelvic adhesions (after obstetric and gynecological surgery, colectomy, or appendectomy).
There are about 10-20% of small bowel obstruction due to hernia. Malignant (secondary) tumors account for about 10%. The remaining nuclei are more rare: intestinal tuberculosis, gallstones, benign tumors, foreign bodies, food residues.
Small bowel obstruction can be classified according to the degree of intestinal obstruction (complete or semi-obstructed) or classified according to the perfusion status of the obstructed segment of the intestine (simple obstruction or strangulation).
2. Clinical symptoms of small bowel obstruction

Người bị tắc ruột non thường có biểu hiện đau bụng quặn từng cơn
3. Diagnosis of small bowel obstruction
3.1 Physical examination Whole body: The patient has signs of dehydration, the degree of dehydration depends on the time of obstruction Signs of abdominal distention are always present (except for high intestinal obstruction) If the patient has old surgical scars on the abdominal wall: Signs Signs suggestive of intestinal obstruction due to adhesions Manifestations of bowel loop dilatation and increased spasm: Floating loop sign, snake sign, auscultation of bowel sounds with increased tone and frequency Abdominal examination without focal pain, palpable A mass (tumour, tuberculosis) is seen. Inguinal examination (to diagnose the cause of strangulated hernia) and rectal examination (lower bowel obstruction due to rectal tumor). 3.2 Subclinical diagnosis Unprepared abdominal radiograph: The first indication for hospitalized patients with intestinal obstruction syndrome. This is a test with relatively high diagnostic value. X-ray of small intestine with Barium: Indicated in cases of high intestinal obstruction or semi-obstruction Ultrasound: With early bowel obstruction, ultrasound has diagnostic value. higher than the abdominal radiograph. CT, MRI: Have high diagnostic value. Rarely indicated in general bowel obstruction, except for the following cases: Intussusception due to intussusception, intestinal obstruction due to tumor, unknown diagnosis of intestinal obstruction, suspected intestinal strangulation, high suspicion of intestinal obstruction, suspected obstruction postoperative bowel. Tests: Electrolyte concentration, Hct, BUN .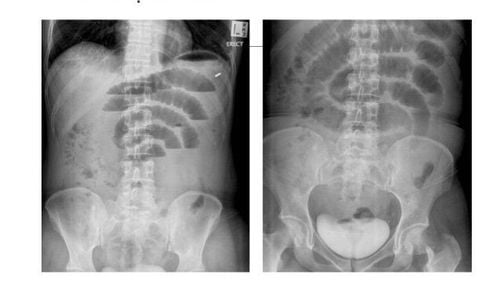
Hình ảnh chụp X-Quang tắc ruột
4. Treatment of small bowel obstruction
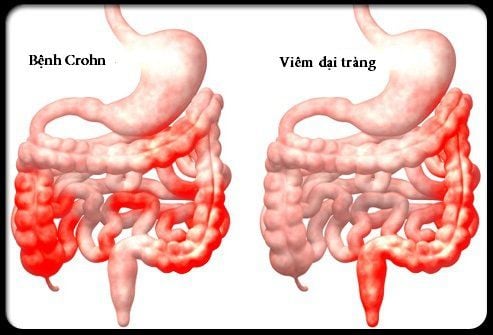
4.1 Medical treatment Medical treatment is indicated in the following cases:Semi-obstruction of small intestine due to adhesion Semi-obstruction of small intestine due to inflammatory bowel disease (Crohn's disease, intestinal tuberculosis,...) Complete small bowel obstruction due to adhesions and Patients arrive early (before 6 hours) The medical treatment process is carried out including:
For the patient to fast, can put a nasogastric tube or small intestine for decompression Rehydration of fluids and electrolytes X-ray Unprepared abdomen every 6 hours (if due to adhesions) or every 24 hours (if due to inflammation) to assess progress of bowel obstruction. The radiographic signs showed good progress: the bowel was less distended, the abdomen was slightly translucent, and the colon appeared slightly. Clinical examination many times, clinical signs showed good progress: abdomen flattened, defecation, appetite. Medical treatment fails if condition does not improve after 48 hours
4.2 Surgical treatment

Phẫu thuật để điều trị tắc ruột non
Complete small bowel obstruction, regardless of cause Obstruction or semi-obstruction of small intestine due to adhesion, failure of medical treatment Obstruction or semi-obstruction of small intestine due to tumor Cannot exclude intestinal strangulation Principles of surgery:
General anesthesia Midway laparotomy Find the site of intestinal obstruction Check the entire small intestine and large intestine Intestinal obstruction due to adhesions: Remove adhesions, cut the adhesive cord, release the sticky bowel loops that are at risk of causing later on. Intestinal obstruction due to tumor: Removal of the bowel with tumor, end-to-end anastomosis Intestinal obstruction due to gallstones: Push the stone to the upper dilated intestine, open the intestine to remove gallstones Intestinal obstruction due to food residues: If the pulp is soft, push the pulp through the ileocecal valve, down to the colon. If the pulp is large and firm, push the pulp to the upper dilated intestine, open the intestine to remove the residue. Laparoscopic surgery for small bowel obstruction due to adhesions:
Indications in certain cases Laparoscopic surgery has many advantages over open surgery, the possibility of success depends on the experience of the surgeon and the level of surgery. degree of abdominal distension, degree of adhesion, number of adhesions. Master. Doctor Vu Huy Binh has 09 years of experience in the field of Gastrointestinal Endoscopy. Currently working as a Gastroenterologist at the Department of Medical Examination & Internal Medicine - Vinmec Hai Phong International General Hospital.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.