This is an automatically translated article.
The article is professionally consulted by Master, Doctor Ta Quang Hung - Department of General Surgery - Vinmec International General Hospital Da Nang.Anesthesia to put Laryngeal Mask is a technique that is very suitable for ophthalmic surgery. Among them, there is an orbital floor lift surgery due to the convenience and nature of controlling the airway much easier than an endotracheal tube.
1. Learn about orbital floor lifting surgery and laryngeal mask anesthesia in orbital floor lifting surgery
1.1 What is the orbital floor?
The floor of the orbit (or orbit) is a thin layer of bone separating the orbit from the maxillary sinus, supporting the eyeball and surrounding tissues.The floor of the orbit is also the most common site of injury, causing rupture of the orbital floor, leading to the eyeball and surrounding structures being stuck into the fracture socket, herniating into the maxillary sinus, causing dangerous complications. Dangers such as: Double vision, ophthalmoplegia causing strabismus, concave eyes, seriously affecting aesthetics, so it is necessary to have early surgery within 2 weeks after the injury.
1.2 Why is laryngeal mask anesthesia indicated in orbital floor lift surgery?
Laryngeal mask anesthesia in strabismus surgery helps control breathing, patients lose pain sensation during surgery. This is a simple method, with few complications, and can be removed early for patients with ophthalmic diseases. The mask can be removed while the patient is still under anesthesia (in the case of not using muscle relaxants), removing the mask early to avoid causing irritation to the patient, this is an advantage of placing a laryngeal mask in ophthalmic surgery to avoid irritation. increase intraocular pressure. Anesthesia to put the Laryngeal Mask is an easy technique to perform, does not require a lot of experience, little stimulation when removing the tube, is very suitable for ophthalmic surgery.
Gây mê mask thanh quản giúp kiểm soát hô hấp trong suốt cuộc phẫu thuật
2. Indications and contraindications for laryngeal mask anesthesia in orbital floor lift surgery
Indications:Patients with contraindications to anesthesia for strabismus surgery. Anesthesia does not guarantee pain control for surgery. Patients with neuromuscular disease cannot use muscle relaxants during endotracheal anesthesia. Patients with indications for endotracheal anesthesia predict difficult intubation, or failed intubation. Contraindications
Insufficient means of resuscitation. The operator has little experience and is not technically proficient. Contraindicated with the use of Laryngeal Mask.

Bệnh nhân có tăng áp hốc mắt được chỉ định trong gây mê mask thanh quản trong phẫu thuật nâng sàn hốc mắt
3. Steps to administer laryngeal mask anesthesia in orbital floor lift surgery
Step 1: Vacuum the ball, lubricate the back of the mask.Step 2: Initiate anesthesia deep enough. Most start with fentanyl followed by a sedative (Propofol, volatile anesthetic), and a muscle relaxant if necessary.
Step 3: Have the patient tilt his head as much as possible, open his mouth.
Step 4: Put the laryngeal mask. Insert the laryngeal mask through the mouth, lean the back of the mask to slide along the hard palate, place the tip of the index finger of the dominant hand at the junction between the tube and the ball, push the mask down to the lower throat until resistance is felt. Inflate the balloon with enough air while not holding the tube so that the mask stays in place.
Step 5: Fixed, check the position of the mask. When the mask is in position, inflate the cuff. Then check if the mask is in the correct position. Finally proceed to fix the tube with two strands of adhesive tape.
Step 6: Maintaining anesthesia can be self-breathing or controlled breathing depending on the case. Monitor parameters when maintaining anesthesia: pulse, blood pressure, SpO2, EtCO2 (CO2 pressure at the end of expiration).
4. Notes during anesthesia mask laryngeal mask
Difficult to place: Do not try to push, check that the head of the laryngeal mask does not roll, lean against the back wall of the pharynx, let the head tilt to the maximum, push the lower jaw forward. In addition, the cause of failure to put the mask on is because the anesthesia is not deep enough, so the anesthesia is deep enough to reset the mask. Attention should be paid to gentle movements to avoid injuries when putting on the mask due to too rough movements. Detecting misplacement by auscultation can detect laryngeal stridor. Note that the laryngeal mask tube is folded, the mask is lowered, the mask is out of position, it is necessary to monitor respiratory parameters to detect early folding and lowering of the laryngeal mask. Complications caused by muscle relaxants (if used), morphine: relax muscle and stop morphine antagonists in time.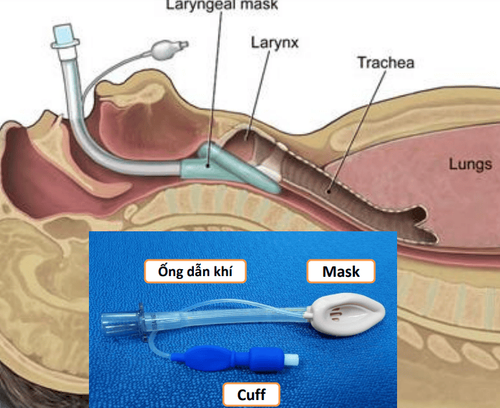
Trong quá trình gây mê mask thanh quản, lưu ý động tác nhẹ nhàng tránh các chấn thương khi đặt mask do động tác quá thô bạo.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
LEARN MORE
Surgery on top of the eye socket Tips to keep myopia from increasing degree 8 ways to treat dark eyes due to lack of sleep