This is an automatically translated article.
The article was professionally consulted by an eye doctor - Department of Examination & Internal Medicine - Vinmec Hai Phong International General HospitalThe floor of the orbit is a thin layer of bone separating the eye socket from the maxillary sinus, which supports the eyeball and surrounding organization. This is the most common site of injury in the walls of the orbit because of the very thin bony structure.
1. Orbital bone structure
The orbit is a pear-shaped bone that is made up of 7 bones: the maxillary bone, the cheekbone (XGM), the frontal bone, the lacrimal bone, the palatine bone, the ethmoid bone, and the sphenoid bone. Orbital dimensions are as follows: orbital volume is 3cm3, orbital margin height is 40mm, orbital margin width is 35mm, orbital depth is 40-50mm, distance from posterior eyeball to eye hole angle is 25mm.
Ceiling of the orbit (superior wall): formed by the frontal bone and the small wing of the sphenoid bone, with the outer lacrimal fossa joining the structure of part of the anterior skull base.
Outer orbital wall: formed by the frontal process of the cheekbones, the frontal bone and the great wing of the sphenoid bone, with the orbital tubercle (Whinal) is the attachment site of the orbital ligament. This wall has a frontal-cheek joint that is easily broken when the bone is broken above the cheekbone.
Intraorbital wall: formed by the ascending maxillary bone (XHT), the paper bone and the sphenoid body, located next to the ethmoid sinuses, sphenoid sinuses and nasal cavities. The inner part of the orbital wall is very fragile, and the tear duct is easily damaged.
Orbital floor (lower wall): formed by the maxillary bone, cheekbone and palatine bone, with grooves and recesses below the orbit. The floor of the orbit is thin, the upper surface of the maxillary sinus. In fractures on the cheekbones, this wall is prone to collapse and the soft tissue below and on both sides of the eyeball is easy to fall into the maxillary sinus, deflecting the eyeball axis, or indenting the eyeball downwards.

Ổ mắt là một hốc xương hình quả lê được cấu tạo nên bởi 7 xương
Slits and holes
Superior orbital fissure: is the part between the wings of the large butterfly and the small butterfly, through which the III, IV, and VI cords and the first branch (branch) of the V cord and sympathetic fibers pass. Inferior orbital fissure: bounded by the sphenoid bone, maxillary bone, and palatine bone and located between the outer wall and floor of the orbit. This cleft contains the second branch (maxillary branch) of the V cord, the zygomatic nerve. The infraorbital nerve (branch of the maxillary nerve) enters the suborbital sulcus and the infraorbital canal and supplies sensation to the lower eyelids, cheeks, upper lip, and maxillary teeth. Fracture of one-third of the orbital floor is usually associated with according to sensory disturbances in the dominant region of the orbital cord. Nasal nasolabial fold: goes from the fossa of the lacrimal gland down to the lower nasal passage. optic canal: the optic canal is 8-10mm long, located in the small wing of the sphenoid bone, separated from the superior orbital fissure by the bony wall. The optic nerve, ophthalmic artery, and optic nerve all pass through the optic canal. The tip of the tube on the orbital side is called the optic foramen. When trauma fractures on the cheekbones, breaks and collapses posteriorly of the orbital wall, the optic canal may collapse, bone fragments, hematomas, swelling around this area are easy to compress or break the optic nerve. affect vision to varying degrees.
2. Intraorbital soft tissue components
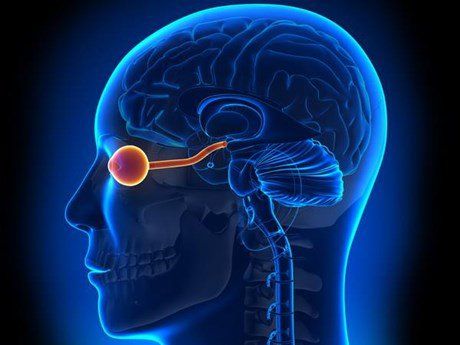
Intraorbital optic nerve: the segment of the optic nerve in the orbit is calculated from the visual hole to the posterior pole of the eyeball, 25 - 30mm long, slightly overlapping and curving the letter S to be able to move according to the eye bridge.
Ring of Zinn: is a fibrous ring formed by the common origin of the axial muscles. The ring of Zinn encloses the optic foramen and the medial portion of the superior orbital fissure. The hole formed by the ring of Zinn is called the ophthalmic foramen, through which cords III, VII, IV and the ophthalmic branch of cord V pass.
Ocular muscles: oculomotor muscles create movement of the eyeball and eyelids: 4 axial muscles come from the ring of Zinn, the levator muscle comes from above the ring. When trauma to the orbital bone fracture, this muscle system can be paralyzed, stuck in the gap between the two bones, causing strabismus or limited eye movement in a certain direction.
Tear gland: located in the frontal fossa above the orbit, including a large lobe in the orbit and a small lobe in the eyelid. The ducts originate from the two lobes of the eyelids and drain into the conjunctiva and the outer superior map.
Orbital fat: is the tissue that acts as a cushion to protect the eyeball and eyelids. Fat masses are located behind the orbital wall and in front of the sphincter.

Đoạn thần kinh thị giác trong ổ mắt được tính từ lỗ thị giác đến cực sau nhãn cầu
3. Eyelids
Eyelid skin: This is the thinnest skin on the body and there is no subcutaneous fat layer. The layer of cushion under the skin is very loose, making it easy for the eyeball to move regularly. The upper eyelid crease is about 8-11mm from the free edge of the eyelid (depending on race). This fold corresponds to the place where the levator fascia attaches to the ciliary sphincter bundles and is also located near or across the upper margin of the blepharitis. There is also an eyelid crease on the lower eyelid, but it is not obvious, sometimes it is just a small ridge that forms the boundary between the skin of the eyelid cartilage and the skin of the eyelids.Each upper and lower eyelid skin is an aesthetic unit of the eyelid. When doing eyelid plastic surgery, attention should be paid to respecting the eyelid folds and the eyelid aesthetic unit.
The muscles that move the eyelids:
The muscles that close the eyelids: the ciliary arch muscle is the main muscle that closes the eyelids, when the muscle contracts, it narrows the cleft. The sphincter muscle is divided into three parts: anterior to cartilaginous, anterior orbital, and anterior septum. The anterior cartilaginous and anterior septal parts participate in automatic eyelid movements, the anterior orbital part participates mainly in automatic eyelid movements, and the active movement is closing the eyes. The muscles that lift the eyelids: include the levator muscle and the upper cartilaginous muscle (Muller muscle). The levator muscle originates from the apex of the orbit just above the ring of Zinn, radiating from the top down to the margin of the ciliary cartilage. The Muller muscle is located behind the levator fascia, descends downwards and adheres along the superior border of the upper eyelid cartilage. The Muller muscle can lift the upper eyelid by 2mm, if it is paralyzed, it can lead to a slight drooping of the eyelids (Horner's syndrome). Eyelid cartilage: is a sheet of connective tissue that acts as a framework of the eyelids, it attaches to the periosteum on the inside and outside. Upper eyelid cartilage is 10-12mm wide, while lower eyelid cartilage is only 4mm wide. Eyelash cartilage is 1mm thick and tapered to both ends.
Conjunctiva: is a non-keratinized squamous epithelium, with two conjunctival parts, the ciliary conjunctiva and the ocular conjunctiva. Angle formed by two conjunctival parts forming the same map.
4. Blood vessels, orbital nerves
Vascular system:
The main source of supply to the orbit is the ophthalmic artery (branch of the internal carotid artery), partly from the internal maxillary artery and the facial artery (branch of the external carotid artery). The ophthalmic artery has many rings that connect to the external carotid artery through the orbital ring. The superior ophthalmic vein is the main drainage vein of the orbit, it originates from the upper part of the orbit, goes behind the superior orbital fissure, and empties into the cavernous sinus. Nerve:
Sensation for the periorbital area is the eye branch and the maxillary branch of the V cord. The muscles of the eyelid sphincter, the muscle of the nasal pyramid, the muscle of the eyebrows, the muscle of the forehead are controlled by branches of the VII nerve. Sympathetic and parasympathetic nerves control pupillary dilation, tear secretion, skin attachment muscle movement, and eyelid vascular dilation.

Bệnh lý về mắt rất thường gặp
5. Angle ligament
The shape of the pterygium is maintained by the medial angle ligament and the lateral oblique ligament. The medial angle ligament attaches to the anterior and posterior lacunae, when it reaches the outside of the lacrimal sac to merge into one, then separates into the superior and inferior branches to attach to the upper and lower eyelid cartilages. The lateral orbital ligament attaches to the lateral orbital tubercle on the medial surface of the orbital margin, dividing into two branches into the upper eyelid cartilage and the lower eyelid cartilage. In periorbital trauma, the most common are the two corners of the eye. When performing surgery in the corner of the eye, it is also necessary to pay attention to avoid damage to the ligaments, if it is necessary to intervene, carry out the reconstruction of the angle ligament to maintain the balanced shape of the eyelid slits of the two eyes.
7. What is orbital bone fracture?
The eye socket is a solid structure, connected by seven bones and creating four different areas. Orbital fractures can occur in any one of these areas, producing various injuries:
Orbital rim fractures: these fractures occur at the outer edges of the orbit. The rim of the eye socket is very thick, so only extreme force such as trauma from a car accident can break it. This force can also damage the nerves, muscles, and connective tissues in the eye. Direct orbital floor fracture: An orbital rim fracture may extend to the orbital floor, causing a direct orbital floor fracture. This usually happens as a result of a serious injury. Indirect orbital floor fracture: Also known as orbital fracture, indirect orbital floor fracture usually occurs when an object such as a handlebar, fist, baseball, or elbow hits the eye socket. These effects do not affect the orbital rim but cause a hole in the floor of the orbit. This hole can block muscles, nerves, or other tissues, making it difficult for the eyes to move and causing vision problems. Portal fracture: A fracture usually occurs only in children because their bones are softer - this is a type of fracture in the eye socket. Instead of breaking, the bones bend outward, then flip back to their normal position. Although not exactly a common fracture, a portal fracture can still lead to serious and sometimes permanent damage. Vinmec International General Hospital with a system of modern facilities, medical equipment and a team of experts and doctors with many years of experience in medical examination and treatment, patients can rest assured to visit. and hospital treatment.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.