
This is an automatically translated article.
The article was professionally consulted by Specialist Doctor I Nguyen Duc Thong - Anesthesiologist - General Surgery Department - Vinmec Danang International Hospital.Compared with anesthesia, anesthesia is a pain-relieving method during childbirth that brings many advantages, spinal anesthesia is a pain-relieving technique performed before a cesarean section to help pregnant women pass labor easily, without feeling any pain. feel pain. In this article, some current up-to-date reviews of the prevention and management of hypotension after spinal anesthesia for cesarean section are presented.
1. What is spinal anesthesia?
Spinal anesthesia is currently the most common anesthetic method in cesarean section. Maternal hypotension is a common complication following spinal anesthesia with adverse consequences for the mother and the fetus. Prevention and treatment of hypotension after spinal anaesthesia continues to be studied.2. Complications of spinal anesthesia
2.1. Neurological complications Paralysis, nerve damage: This is a very rare complication. There are many causes of post-anesthesia nerve damage, such as: needle/catheter, compression, epidural hematoma, ischemia, or toxicity of the anesthetic on the nerve. Usually, in addition to the loss of pain sensation, the patient will also experience paralysis of the area being numbed. However, movement and sensation will recover after the effect of the anesthetic has worn off (about 4-6 hours). If these symptoms persist, notify your healthcare provider immediately. Cauda equina syndrome: Usually has symptoms of low back pain, numbness around the anus and urinary incontinence. Headache: This is a common symptom after spinal anaesthesia, which usually resolves on its own within 7 days. If symptoms cause significant discomfort, pain relievers can be used. In case the headache does not go away on its own within 7 days or the headache is severe, it is necessary to immediately seek medical assistance. To prevent headaches after spinal anaesthesia, the patient should lie still in bed for 24 hours after anesthesia and do not raise their head.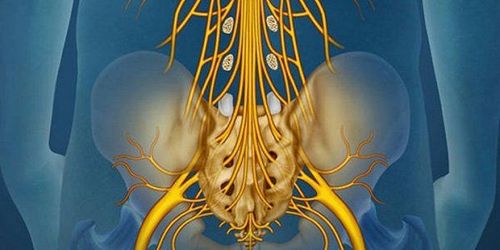
Hội chứng chùm đuôi ngựa là biến chứng về thần kinh có thể gặp sau khi gây tê tủy sống
2.4. Infections An injection of local anesthetic into the spine can cause meningitis or an epidural abscess. However, this complication almost does not occur because it is very well prevented by aseptic measures during the procedure.
2.5. Back pain After CNS anaesthesia, some patients feel back pain at the injection site. This symptom can be improved by using the smallest needle possible (choose the 29G needle), avoiding repeated needle puncture by using ultrasound to identify the vertebral space before anesthesia, possibly using analgesics.
2.6. Urinary retention Local anesthetics can inhibit the nerve roots that regulate urine secretion. Therefore, patients often feel urinary retention after surgery. This symptom can be solved by massaging the lower abdomen, applying heat to the bladder area; If you are unable to urinate, a catheter (tube that carries urine) is placed to drain the urine. After the effect of the anesthetic wears off, urinary retention may improve.
2.7. Itching may occur after spinal anesthesia if the doctor adds a morphine pain reliever to the anesthetic to increase the duration of action. This sign usually improves on its own.

Tình trạng bí tiểu thường gặp sau khi mổ lấy thai
3. Treatment and prevention
3.1. Infusion Although the use of intravenous fluids is considered a classic in the practice of obstetric anesthesia, recent evidence has questioned its validity. Some authors have reported that spinal anesthesia in the obstetric population is accompanied by an increase rather than a decrease in cardiac output. This finding makes perfusion for the prevention of hypotension following spinal anaesthesia not as hypothesized. Furthermore, maternal infusion has been reported to disrupt glycocalyx. Glycocalyx is a carbohydrate-rich layer lining the endothelium that plays a role in maintaining endothelial integrity. Destruction of endothelial glycocalyx has been reported as a cause of failure to administer fluids to prevent hypotension after spinal anesthesiaPre-infusion: although prior crystalloid infusion is superior to no-infusion regimen, the rate hypotension with all prior infusion regimens remained elevated. According to the latest assessment from the Cochrane database, pre-infusion of colloidal solution is better than crystalloid infusion; however, randomized controlled studies comparing colloids and pre-infusion crystals show conflicting evidence.
Concurrent infusion: the currently accepted explanation for the pre-infusion limit value is rapid distribution of fluid in the extravascular space. This is the cause of the development of the concept of simultaneous infusion of fluids in which fluids are given rapidly concurrently with spinal anesthesia. With simultaneous rapid infusion of fluids, redistribution of fluid can be limited by concomitant vasodilatation.
Most reports show that concurrent infusion is superior to (or at least the same as) infusion before comparing two protocols using the same fluid. Concurrent crystalloids are superior to pre-infusion crystals and are comparable to pre-infusion colloids. Colloidal infusion at the same time is no better than colloidal infusion first.
Compared with different fluids, crystalloids infused at the same time are similar to colloids given at the same time. However, the volume of fluid required with colloid is less than the volume of crystalloid.

Thuốc co mạch có thể làm giảm hạ huyết áp sau tê tủy hơn truyền dịch
Bradycardia (Initial bradycardia or hypotension after myelosuppression associated with bradycardia): Adverse effects of phenylephrine: The effect on maternal cardiac output makes ephedrine the drug of choice in cases of bradycardia-related bradycardia. Patients with compromised cardiac function: Although there are no studies comparing both drugs in this population, their effects The adverse effect of phenylephrine on cardiac output is still considered to limit its use in these patients Placental dysfunction: Phenylephrine reduces maternal cardiac output and increases peripheral vascular resistance, and by which reduces uterine perfusion. In only one randomized controlled clinical trial conducted in pregnant women with fetal distress, there was no difference between ephedrine and phenylephrine in Apgar scores and cord blood pH.

Trước mổ lấy thai cho sản phụ nằm nghiêng trái có thể giúp giảm chèn ép động mạch chủ
Most poses have one of two goals as follows:
Reduce aortic compression Increase venous return to Vinmec International General Hospital is one of the hospitals that strictly apply practice standards safe surgical anesthesia according to international guidelines. With a team of experienced anesthesiologists and nurses, along with modern equipment such as nerve detectors, ultrasound machines, Karl Storz difficult airway control system, anesthesia monitoring system GE's comprehensive AoA (Adequate of Anesthesia) including monitoring of anesthesia, pain and muscle relaxation will deliver high quality and safety, helping patients to have adequate anesthesia, not awake, no residual relaxant muscle after surgery. Vinmec Health System is also proud to be the first hospital in Vietnam to sign with the World Anesthesiology Association (WFSA) towards the goal of becoming the safest hospital for surgical anesthesia in Southeast Asia.
If you have a need for consultation and examination at Vinmec Hospitals under the nationwide health system, please book an appointment on the website for service.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.













