This is an automatically translated article.
The article is professionally consulted by Master, Doctor Nguyen Ngoc Thang - Gastroenterologist - General Surgery Department - Vinmec Danang International General Hospital. The doctor has 17 years of experience in the field of gastrointestinal and hepatobiliary surgery, and has over 9 years of experience in endoscopic intervention.Esophageal varices is one of the complications of portal hypertension that is common in patients with cirrhosis mainly due to alcohol. Esophageal varices can be detected endoscopically, and in severe and severe degrees can rupture and cause gastrointestinal bleeding. So how many degrees of esophageal varices?
1. What is esophageal varices?
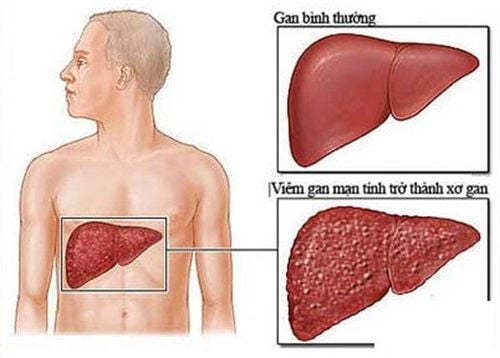
Esophageal varices are common complications in patients with liver disease, especially cirrhosis (due to alcohol, hepatitis B virus, hepatitis C, ...). Cirrhosis causes portal hypertension syndrome and impaired liver function, thereby dilating the esophageal veins.
Esophageal varices, if progressed to a dangerous extent, can rupture and cause severe gastrointestinal bleeding, which can even lead to death. Gastrointestinal bleeding has a risk of recurrence in the following times and leads to blood loss, shock and death, if esophageal varices are not detected and treated in cirrhotic patients.
2. Esophageal varices have how many degrees?
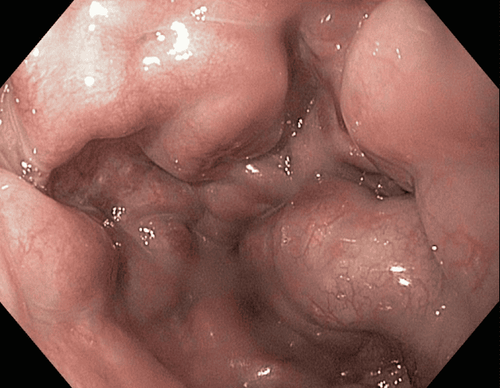
Giãn tĩnh mạch thực quản được phát hiện bằng nội soi
Esophageal varices are graded according to the size of varicose veins.
Grade 1 - Small: The esophageal varices are straight and small. Grade 2 - Moderate: The varicose veins are relatively large in size, stringy in shape and occupy an area of more than one third in the lumen of the esophagus. When inflated, the dilatations do not collapse. Grade 3 - Large: The varicose veins are large in size, shaped like a tumor and occupy an area of more than 1⁄3 in the lumen of the esophagus. However, the American Association for the Study of Liver Diseases (AASLD) has recommended that esophageal varices should be graded into 2 grades: small (varicose size <5mm) and large (variceal size <5mm). dilated >5mm) due to the relatively high rate of dilatations progressing from small to large (7%/year).
To evaluate the progression of varicose veins, doctors rely on the following main factors:
Increased hepatic venous pressure gradient: HVPG >10mmHg Decompensated cirrhosis (Child-Pugh B/C) Cirrhosis Alcoholic liver disease Increased appearance of red lines in the esophageal veins compared with baseline endoscopy.
3. Complications of esophageal varices and prevention and treatment
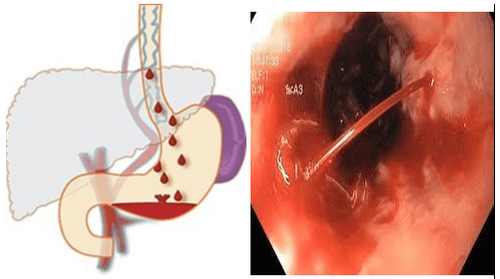
Xuất huyết tiêu hóa do vỡ dãn tĩnh mạch thực quản – hậu quả của giãn tĩnh mạch thực quản không được điều trị
One of the serious complications of esophageal varices is gastrointestinal bleeding. This complication can cause shock and lead to death when the patient loses too much blood without timely detection and treatment.
However, this complication can be effectively detected and prevented by esophagoscopy. Based on factors that develop varices such as size, red line at endoscopy or not, Child-Pugh grade, the doctor will predict the risk of bleeding and give appropriate treatment.
3.1. Esophageal varices small size, no red line, no bleeding, Child-Pugh grade A Treatment with nonselective beta-blockers slows down the risk of varicose veins formation and progression esophagus and thereby limit bleeding. When using beta-blockers, patients do not need to have a repeat endoscopy.
Esophageal endoscopy is performed over 1 - 2 years (1 year if disease factors have not been eliminated and 2 years if disease factors have been eliminated) in patients not on beta-blocker therapy to promptly detect red lines in the esophageal veins or the progression of varicose veins.

Điều trị búi giãn tĩnh mạch thực quản bằng thuốc chẹn beta giúp làm giảm nguy cơ hình thành và tiến triển bệnh
3.2. Esophageal varices small in size, with red lines, without bleeding, Child-Pugh grade B/C The main treatment for esophageal varices is the use of non-selective beta-blockers (nadolol, propranolol) at the maximally tolerated dose.
3.3. Esophageal varices of medium to large size, no red lines, no bleeding, Child-Pugh class A Non-selective beta-blockers (eg, nadolol, propranolol) or alpha-blockers are recommended. -adrenergic (carvedilol) in patients with moderate to large esophageal varices and not at high bleeding risk.
Consider endoscopic rubber band ligation therapy in patients with contraindications to, rejection of, or intolerance to beta-blockers.
3.4. Esophageal varicose veins of medium to large size, red streaked, non-bleeding, Child-Pugh grade B/C For the prevention of primary bleeding in patients with true varicose veins In patients with moderate to large management and high risk of bleeding, methods include:
Use a non-selective beta-blocker (nadolol, propranolol) or a non-selective beta-blocker - alpha-adrenergic blocker (carvedilol) In addition to preventing bleeding, the drug also has a good effect on reducing the spread of bacteria, thereby reducing the risk of peritonitis, primary infection, ascites and hepatorenal syndrome. Laparoscopic rubber band ligation: This procedure should be performed for 2 to 3 weeks until the esophageal varices are completely removed. Then, follow up by endoscopy 3, 6, 12 months. 3.5 Treatment of gastrointestinal bleeding due to rupture of esophageal varices

Trường hợp xuất huyết tiêu hóa do biến chứng vỡ giãn tĩnh mạch thực quản cần sử dụng thuốc co mạch để làm chậm lưu lượng máu chảy vào tĩnh mạch cửa
When esophageal varices rupture and cause bleeding, this condition should be controlled and prevented early to limit the risk of shock and death to the patient.
Management and treatment of bleeding complications due to rupture of esophageal varices include the following techniques and methods:
Hemostasis and blood volume replacement by transfusion of blood and blood products. Use vasopressors to slow blood flow into the portal vein. The drug can be used for 3 to 5 days after bleeding and during endoscopy. Endoscopy for diagnosis, identification and ligation of varicose veins with an elastic band. In case the treatment of elastic band ligation of esophageal varices fails, it is necessary to perform TIPS method - intrahepatic portal opening through the jugular vein. Control bleeding using balloon catheters or metal stents. Take antibiotics to prevent infection in the bleeding. Liver transplant surgery in patients with recurrent bleeding or advanced liver disease. This method is highly effective if a suitable liver transplant is found. Esophageal varices are classified into 2 basic levels, small and large, based on the size of the varicose veins. Esophageal endoscopy is a method to help detect and prevent esophageal varices from rupture causing bleeding.
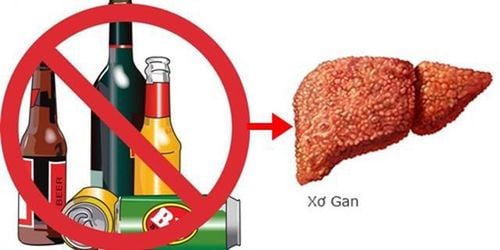
To prevent esophageal varices due to cirrhosis, in addition to regular check-ups and medication use as prescribed by the doctor, patients need to maintain a scientific and healthy lifestyle:
Should limit the following items alcoholic beverages such as alcohol because these are harmful to the liver Eat healthy, apply a diet suitable for people with cirrhosis such as eating more fruits and vegetables, limiting fat and salt,. Should regularly monitor to maintain weight and regularly exercise to improve physical fitness. In particular, cirrhotic patients need regular check-ups and blood tests to evaluate liver - biliary function periodically. Cases of high-risk patients need to go to a medical facility for timely monitoring, diagnosis and treatment.
With many years of experience in the examination and treatment of diseases, Vinmec International General Hospital has become one of the major health care centers, capable of examining, screening and treating patients. many diseases in the gastrointestinal tract such as hepatobiliary - pancreas - esophagus. Therefore, if there are signs of esophageal dilation and a history of gastrointestinal disease, you can take your child to Vinmec International General Hospital for examination and support and advice from doctors.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.