This is an automatically translated article.
The article was professionally consulted by Specialist Doctor I Tran Thi Anh Hien - Department of Surgical Anesthesia - Vinmec Central Park International Hospital, Master, Doctor Ta Quang Hung - General Surgery Department - Hospital Vinmec International General Hospital Da Nang.Intubation is a difficult anesthetic technique and carries a high risk of complications. Therefore, the implementation of the endotracheal intubation procedure should be prescribed by specialized doctors at qualified medical facilities.
1. What is intubated anesthesia?
Endotracheal anesthesia is a technique of general anesthesia with endotracheal intubation for the purpose of respiratory control during surgery and postoperative resuscitation. During surgery, under the effect of anesthesia, the patient will temporarily lose sensation and consciousness, but the patient can still breathe on his own or breathe with a machine through an endotracheal tube. Accordingly, anesthesia with intubation has the following benefits:Helps maintain upper airway ventilation for the patient. Makes bronchial aspiration easy. Make it easy for the doctor to provide supportive or commanding breathing. In addition, tracheal intubation also ensures breathing during general anesthesia in different positions, in critical stages and in postoperative resuscitation.
2. Indications and contraindications of endotracheal anesthesia

Chống chỉ định với phương pháp gây mê nội khí quản khi bệnh nhân bị ung thư thanh quản
The method of endotracheal anesthesia is indicated in the following cases:
Cases of deep organ surgery, major surgeries, in need of muscle softening. Cases of patients with shock, multiple trauma. Thoracic surgery, cranial surgery. Surgery on a patient with a full stomach. In the case of respiratory control with a mask, it is difficult. Surgery with abnormal posture such as in maxillofacial surgery, head and neck surgery, side or prone position. Cases requiring maintenance of anesthesia with inhalational anesthetics for spontaneous breathing in young children and neonates. Endotracheal anesthesia is absolutely contraindicated in the following cases:
Medical facilities do not have enough resuscitation facilities. There is no qualified person to do it. Endotracheal anesthesia is relatively contraindicated in the following cases:
Patients with acute inflammation of the upper respiratory tract. Patient has severe laryngeal tuberculosis. Patient has laryngeal cancer.
3. Intubation procedure
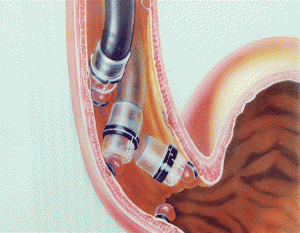
Kỹ thuật đặt nội khí quản cấp cứu
To achieve high treatment results, it is necessary to fully comply with the steps in the technique of anesthesia intubation. First prepare:
Prepare stethoscope, suction machine, check pulse, temperature, blood pressure for the patient. Prepare anesthetic agents. Give the patient 100% oxygen for at least 3 minutes. Step 1: Initiation of anesthesia:
Most start with Fentanyl Sleep-inducing drugs such as Thiopental, Propofol, Etomidate, Ketamine. Muscle relaxants such as: Norcuron, Succinylcholine, Pavulon, Arduan Tracrium. Muscle relaxants should be injected only when mask breathing has taken effect. Regarding the dosage of the drugs used according to the dose of intravenous anesthetic. Step 2: Local anesthesia
Local anesthesia is performed by using Xylocaine 5% spray after the laryngoscope is brought to the patient's epiglottis.
Spray into the glottis 4 - 7 times. Spray on the sound bar 4 - 7 times. Spray into the trachea 4-7 times. These three positions spray a maximum of no more than 25 times.
Step 3: Perform intubation technique
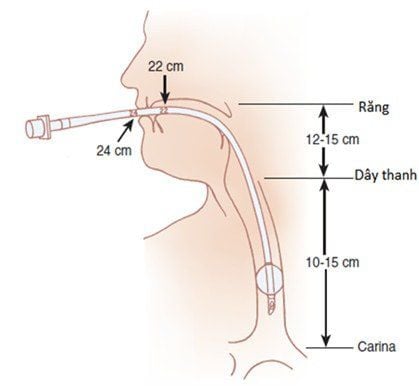
Oral intubation Place the patient in a supine position, so that when looking at the mouth, the pharynx and larynx are on the same axis. The most commonly used pose is from the modified Jackson pose: the knees are 8 - 10cm higher than the shoulders. The operator holds the laryngoscope in the left hand, and the right hand opens the patient's mouth. It is necessary to open the patient's mouth wide to avoid damage to the lower lip, to avoid the obstruction of the teeth and tongue when the lamp is inserted. The lamp is inserted into the right lip, then gradually pushed down along the tongue, along the midline and pushed the tongue to the left, until the tip of the lamp reaches the position of the lingual lingual - epiglottis. Raise the lamp high and gently move forward until the glottis is visible. Next, the right hand or an assistant will press or gently push the thyroid cartilage to the side so that the glottis can be seen. Then insert the endotracheal tube into the right corner of the lip and then into the glottis. After the balloon of the endotracheal tube passes about 2 cm over the vocal cords, it stops. Use a 10ml syringe to inflate the balloon, the amount of air is just enough to not leak during respiration. Then the laryngoscope will be gently taken out. Hold the endotracheal tube close to the edge by clamping between thumb and index finger. Perform manual respiration and check the position of the endotracheal tube for correct position by listening to the lungs and two axillaries. If you can clearly hear the sound of inhalation and exhalation and you can hear the alveolar murmurs on both sides of the lungs, the tube is in place. After determining that the tube is in the correct position, fix it with adhesive tape or a cloth strip. Finally put the canuyn in the mouth to avoid the patient biting the tube. Nasal intubation The catheter is usually inserted through the right nostril, with the beveled edge of the tube toward the nasal septum. The tube is always in a line perpendicular to the face plane. Gently rotate the tube while pushing the tube in to reduce the risk of nasal torsion injury. The combination of local anesthetic and vasoconstrictor increases the diameter of the nostrils and reduces the risk of bleeding. After the catheter is inserted 15 - 16cm, use the laryngoscope as the technique of inserting the light in the above oral catheterization technique. Step 4: Maintain anesthesia:
Depending on each patient's case, it is possible to breathe on their own or breathe with command. In the case of spontaneous breathing with volatile anesthetics, the anesthetic is used and controlled through a special vessel. In case of mechanical respiration or hand squeeze: maintain anesthesia with inhalational anesthetics, combine anesthetics, muscle relaxants, fentanyl by intermittent injection or maintain through an electric syringe. Before the end of surgery, it is necessary to reduce the dose of anesthetic. In case of inhalation anesthesia, it is necessary to stop the drug at the end of surgery, open the valve to the fullest extent, increase ventilation, squeeze the reserve balloon to release the anesthetic during the anesthesia. During the process, it is necessary to monitor the following parameters: Pulse, blood pressure, SaCO2, EtCO2 (CO2 gas in exhaled breath). Step 5: Extubation after endotracheal anaesthesia
Criteria for extubation after endotracheal anesthesia:
● Patient awake, can follow medical orders: open mouth, stick out tongue, Open your eyes, make a fist, lift your head high and hold for 5 seconds.
● The patient can take deep, regular breaths on his own, without needing to be reminded, the breathing rate is >14 times/minute, the tidal volume is 8ml/kg body weight.
● The patient's pulse and blood pressure are stable.
● Sao2 : 98 – 100%.
● Muscle relaxant recovery ≥ 90%
If the patient does not meet the above criteria, the doctor needs to re-evaluate the patient's condition, the effect of muscle relaxants, the respiratory depression of Fentanyl to use muscle relaxants or Naloxone.
Technique for extubation:
Clean the throat and mouth with a sterile suction tube No. 1. Suction a nasogastric tube if available. Remove the endotracheal tube. Insert sterile suction tube 2 into the endotracheal tube, suction and withdraw at the same time. 4. Some possible complications during endotracheal anesthesia Complications encountered during endotracheal intubation: Failure to intubate. Misplaced tube in stomach. Trauma during intubation: tearing lips, broken teeth, hoarseness... Rapid pulse, increased blood pressure during intubation. Complications of folding the tube, retracting the tube, the endotracheal tube is pushed deeply, eliminating one lung. Complications due to muscle relaxants, anesthetics. Endotracheal anesthesia is a difficult technique, it should be performed by highly qualified specialists, and at the same time, medical facilities must have all the necessary equipment to achieve the highest efficiency and prevent possible adverse events.
Vinmec International General Hospital currently has a method of endotracheal anesthesia during surgery performed by a team of skilled and experienced medical doctors, with a system of advanced medical equipment, currently grand.
Graduating from the residency training program, Dr. Tran Thi Anh Hien has experienced many different working environments such as Binh Dan Hospital, Ho Chi Minh City University of Medicine and Pharmacy Hospital and French-Vietnamese Hospital. before returning to work at the Anesthesia and Anesthesia Unit - Department of Surgical Anesthesia - Vinmec Central Park International General Hospital
Master. Doctor Ta Quang Hung has over 10 years of experience in teaching and practicing in the field of Anesthesia and Resuscitation. Currently, working as an Anesthesiology and Resuscitation Doctor, Department of General Surgery - Vinmec Da Nang International General Hospital
For detailed advice on endotracheal anesthesia techniques at Vinmec, please come directly to our office. Contact Vinmec health system or register online HERE.
MORE:
Intubation anesthesia for cesarean section in patients with pre-eclampsia Anesthesia during bronchoscopy Anesthesia, pre-anesthesia: What you need to know