This is an automatically translated article.
The article is expertly consulted by Master, Doctor Ton That Quang - Head of Anesthesia - Anesthesia Unit - Department of General Surgery - Vinmec Nha Trang International General Hospital. The doctor has more than 15 years of experience working in the Anesthesia - Resuscitation industry.Thoracic fistula is one of the relatively uncommon operations in thoracic surgery. With advances in medical technology, thoracic fistula suture can now be performed endoscopically under endotracheal anesthesia.
1. Overview of endotracheal anesthesia for thoracic fistula suture
Endotracheal anesthesia is a technique that uses anesthetic drugs under the general route. At the same time, the patient's respiratory function was actively controlled by double-lumen intubation. At the same time, during the surgery, the patient is also used sedation, pain reliever and muscle relaxant to facilitate the entire surgery and recovery after surgery.For suturing thoracic duct fistula in thoracic surgery in particular and other endoscopic techniques in general, endotracheal anesthesia is the pre-selected indication with certain advantages and suitability. its. Furthermore, with currently used anesthetics, the onset of action is fast, the effect is rapid, and the adverse effects are minimal in the patient.
However, similar to other surgical interventions, before performing endotracheal anesthesia laparoscopic fistula suture, the patient and family need to be clearly explained the procedure, benefits and risks. The body of the surgery is about to take place. Accordingly, the obvious contraindication of this surgery is when the patient disagrees. On the other hand, due to the requirements of anesthesia, resuscitation, laparoscopic fistula suture under endotracheal anaesthesia cannot be carried out in medical facilities that do not have sufficient facilities, equipment or services. Insufficient human resources, not proficient in techniques, manipulations and improvisations related to surgery.
2. How to conduct endotracheal anesthesia laparoscopic surgery to suture thoracic duct

Hình ảnh máy gây mê kèm máy thở
Patient: Pre-operative examination of anesthesia, assessment of the possibility of difficult intubation, detection and prevention of risk factors for surgery, especially cardiovascular and respiratory function steam. Explain to patient and family to cooperate. Hygiene and fasting according to preoperative procedures. Use sedation the night before surgery if the patient is too nervous. Change the clothes as prescribed and transfer the patient to a sterile area.
Surgical team: including
Doctors, nurses specializing in anesthesiology and resuscitation Specialist thoracic surgeons and surgical assistants Nursing instruments Nursing supporting the outer circumference Means and equipment include:
100% oxygen source Anesthesia machine system with ventilator Life function monitor on 3-lead electrocardiogram parameters, non-invasive blood pressure or arterial blood pressure, SpO2, breathing rate, temperature Machines emergency services such as defibrillators, sputum suction machines... and emergency drugs, vasopressors Endotracheal tubes of all sizes Intubation kits: Laryngoscope, suction tube, mask, squeeze balloon, oropharyngeal cannula, Magill pliers, soft mandrin, balloon inflator and fixation wire. The means of preventing difficult intubation: Cook tube, laryngeal mask, flexible bronchoscope, tracheostomy kit, mouth opener... Local anesthetic: Lidocaine 10% spray. General anesthetic, muscle relaxant sedative. Medical records, pre-operative tests and surgical procedures as prescribed Step 2: Conduct
Check patient's administrative information, records, tests, surgery indications
Prepare pre-anesthesia for patients Patient:
Install means of monitoring blood pressure, electrocardiogram, SpO2... Prepare stethoscope, suction machine. Make a peripheral transmission line with at least 18G needles. Prepare anesthetic and resuscitation medicine. Give 100% oxygen first, at least 3 minutes.
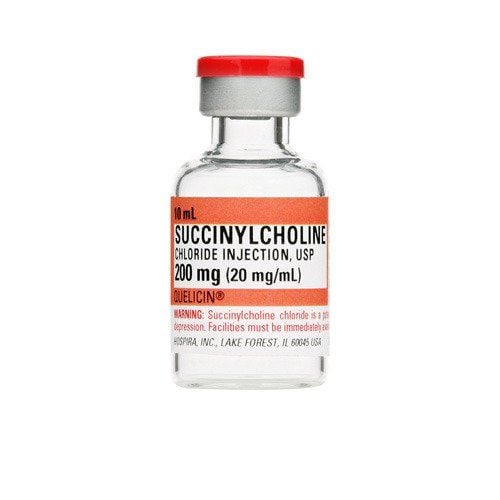
Thuốc giãn cơ succinylcholin chỉ tiêm khi hô hấp bằng mặt nạ đã có hiệu lực
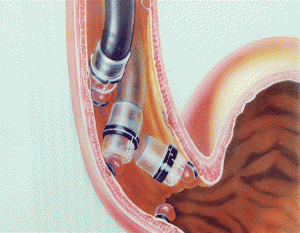
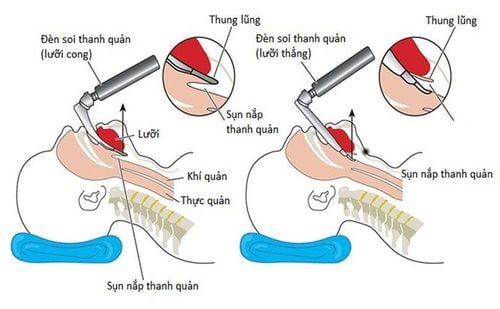
Painkillers: fentanyl, sufentanil, alfentanil... Sleep-inducing drugs (thiopental, propofol, etomidate, ketamine). Muscle relaxants (succinylcholine, norcuron, pavulon, arduan, tracrium) are injected with muscle relaxants only when mask respiration has taken effect. Technique: After induction of anesthesia with sufficient depth and muscle relaxation, let the patient lie on his or her back. Turn on the jaw and put the endotracheal tube up high and gently move forward to slide the tongue to the left, see the glottis (use the left wrist to lift the lamp, do not lean on the teeth, do not pull the lamp handle towards the patient's head). Local anesthetic with xylocaine 5% spray 3-5 times into the trachea. Use the right hand to insert a double-bore endotracheal tube with the spur posteriorly and insert it through the glottis. When the tip of the conduit passes through the retracted vocal cords, Mandrin rotates the endotracheal tube 90 degrees counterclockwise for placement in the left lung and clockwise for insertion in the right lung. While turning and pushing when seeing the entanglement, the spur is now leaning against the tracheobronchial junction. Inflate two Cuff balloons, do not inflate more than 5ml of air for bronchial Cuffs. Connect the 2 tubes of the endotracheal tube with the Y-shaped raccord to ventilate, listen to the alveolar murmur on both sides equally. Take turns clamping 2 Y-branches to control ventilation of each lung. When clamping a Y-branch, the alveolar murmur of the same lung is lost while hearing is still heard on the opposite side. A flexible endoscope can be used to check the position of the endotracheal tube. Secure the endotracheal tube with two adhesive tapes. Put the canun in the mouth to avoid biting the tube. Place a gastric tube. Maintenance of anesthesia:
Endotracheal anesthesia with controlled respiration. Maintain maximal bilateral ventilation when possible. For single lung ventilation: Vt: 8-10ml/kg, f:12-14l/min and maintain Peak airway pressure < 40cmH2O. If SpO2 decreases < 95% then increase FiO2 to 100%, if still decrease then ventilate atelectasis, check tube position, consider PEEP. Respiration by machine to maintain anesthesia by inhalation anesthetic, combination of fentanyl, anesthetic, muscle relaxant by interval injection or maintained by continuous infusion pump. Before the end of surgery, reduce the dose of volatile anesthetics. Aspirating viscous sputum from both endotracheal tube branches completely expands the lungs before closing the chest. When using inhalational anesthetics (sevoran, isofluthan), stop the drug at the end of surgery, open the valve fully, increase ventilation, squeeze the reserve balloon to release the anesthetic during the anesthesia. Monitor parameters when maintaining anesthesia: pulse, blood pressure, SpO2, EtCO2, blood gas. Prevention of endotracheal intubation, tube folding, tube being pushed deep.

Sau khi rút ống nội khí quản bệnh nhân có thể bị viêm đường hô hấp trên
Patient awake, following medical orders: open eyes, open mouth, stick out tongue, clenched fists, hold head high for 5 seconds. Breathe deeply, evenly, without prompting. Breathing rate more than 14 breaths/minute. Tidal volume (Vt 8ml/kg). Pulse and blood pressure are stable. SpO2 98-100%. If the above criteria are not met, the patient's condition must be evaluated, the effect of muscle relaxants, the respiratory depression effect of Fentanyl, the patient still asleep due to the drug, the muscle relaxant or the use of naloxone. Monitoring during anesthesia
Monitoring the depth of anesthesia based on heart rate, blood pressure, sweating, tearing (PRST); MAC, BIS and Entropy (if any)... Monitor vital signs: Heart rate, blood pressure, SpO2, EtCO2, body temperature. Prevent the endotracheal tube from being misplaced, folded, or blocked. Criteria for extubation in the postoperative period The patient was awake and followed orders. Raise the head for more than 5 seconds, TOF > 0.9 (if any). Breathe spontaneously, breathing rate within normal limits. Pulse and blood pressure are stable. Body temperature > 35oC. There were no complications of endotracheal anesthesia and surgery such as mucus obstruction, reflux of digestive juices into the respiratory tract, hemodynamic disturbances due to anesthesia, local trauma due to intubation... In summary, Endotracheal anesthesia is an intraoperative sedation technique that is widely used in most surgeries, including suturing thoracic duct fistulas in endoscopic thoracic surgery. The success of the surgery also depends a lot on the anesthesia work; Accordingly, it is necessary to ensure the necessary requirements of endotracheal anesthesia for the thoracic fistula surgery to take place smoothly.
Vinmec International General Hospital with a system of modern facilities, medical equipment and a team of experts and doctors with many years of experience in medical examination and treatment, patients can rest assured to visit. examination and treatment at the Hospital.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.