This is an automatically translated article.
The article was professionally consulted by Specialist Doctor I Ho Quoc Tuan - Anesthesiologist - General Surgery Department - Vinmec Nha Trang International General Hospital.Surgery for kyphosis scoliosis is a large, complicated surgery with a long time to perform. Endotracheal anesthesia is an anesthetic method used for kyphosis surgery.
1. What is scoliosis surgery?
Scoliosis is a spinal deformity with recognizable features such as: the spine is bent to one side, the shoulders are uneven, the shoulder blades are raised on one side, and the hips are uneven. .. About 10% of cases of kyphosis scoliosis begin when the child is young (0-5 years old), the remaining 90% have late onset at 12-20 years old.
Not only affects aesthetics, kyphosis, if it occurs at a severe level, will greatly affect the health and development of children. When the spine is deformed, it will lead to a change in the volume of the thoracic cavity, the heart and lungs are compressed leading to obstruction of breathing and circulation. Children with lack of oxygen will lead to growth retardation and stunted physical strength. When growing up, health is often weak, not healthy enough to study and work. In addition, children often suffer from diseases such as back pain, degenerative vertebrae, and sclerosis.
Scoliosis is related to genetic factors, due to sitting or sitting in the wrong posture, some types of scoliosis can be caused by cerebral palsy, muscular dystrophy, birth defects spine , injury or infection of the spine.

Bệnh gù vẹo cột sống có liên quan đến yếu tố di truyền
Regarding the treatment of scoliosis, if the disease is mild, the child will be adjusted to the correct sitting position and activities, periodically re-examined every 4-6 months for the doctor to monitor. If the scoliosis is moderate, the doctor will assign the child to wear a brace to correct the scoliosis and prevent further scoliosis. The brace will be worn day and night for a long time, until the young skeleton stops growing. Scoliosis surgery will be indicated in cases of severe and progressive scoliosis. This is a method to correct kyphosis scoliosis by gluing the vertebrae together with spinal manipulation tools combined with autologous bone grafting to keep the spine straight and healthy. Surgery for kyphosis scoliosis is a large, complicated surgery, with a long surgical time, patients at risk of blood loss, hypothermia, and nerve damage after surgery. Endotracheal anesthesia is an anesthetic method used in surgery for kyphosis scoliosis.
2. Endotracheal anesthesia for surgery to correct kyphosis scoliosis
2.1. Point
Endotracheal anesthesia is indicated for patients with kyphosis scoliosis who need plastic surgery or treatment of nerve damage caused by kyphosis. This is a method of general anesthesia with endotracheal intubation.
Endotracheal anesthesia itself is a difficult technique, in patients with kyphosis often have limited or mixed ventilation disorders before surgery. Most kyphosis surgery is performed on the stomach, so the risks such as folding, slipping of the endotracheal tube or nerve damage are higher. Therefore, endotracheal anesthesia is not performed if the patient does not agree or the medical facility does not have enough facilities for anesthesia and resuscitation, and is not technically proficient.
Gây mê nội khí quản phẫu thuật chỉnh gù vẹo cột sống phù hợp với người bệnh có gù vẹo cột sống cần phẫu thuật chỉnh hình thẩm mỹ
2.2. Preparing for endotracheal anesthesia
The person performing endotracheal anesthesia for scoliosis correction surgery is a doctor, a nurse specializing in anesthesiology and resuscitation. Before performing surgery, the doctor will examine the anesthesia, assess the detection and prevent risks. At the same time, explain to the patient the purpose and procedure for the patient to cooperate. The patient will be sedated from the night before surgery if necessary.
Means to perform endotracheal anesthesia include:
Anesthesia machine system with breathing, hand squeeze oxygen source, vital function monitor (ECG indicators, arterial blood pressure, SpO2, EtCO2, etc.) breathing rate, temperature), defibrillator, suction machine,...; Laryngoscope, endotracheal tube of all sizes, suction tube, mask, squeeze ball, oropharyngeal cannula, Magill pliers, soft mandrin; Lidocaine 10% spray, Salbutamol spray; Means should be prepared to prevent difficult intubation: Cook tube, laryngeal mask, flexible bronchoscope, tracheostomy kit, mouth opener,...
2.3. Procedure of endotracheal anesthesia for scoliosis correction surgery
The patient lies on his back, breathes 100% oxygen with a flow rate of 3-6 liters/minute at least 5 minutes before induction of anesthesia. The surgical team installed a monitor and established an effective transmission line. Perform pre-anesthesia if necessary.
Perform induction of anesthesia with drugs:
Sleeping pills: choose one of the drugs such as intravenous anesthetics (propofol, etomidate, thiopental, ketamine,...), volatile anesthetics (sevoflurane, Isoflurane,... ) Painkillers: fentanyl, sufentanil, morphine,... Muscle relaxants: rocuronium, vecuronium, succinylcholine,... are used if necessary. The endotracheal tube will be placed when the patient is in deep sleep with sufficient muscle relaxation (in most cases). Your doctor will choose one of two techniques for intubation: oral intubation and nasal intubation.
Oral intubation technique
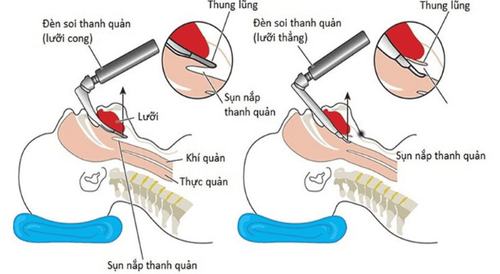
The doctor (or anesthesiology specialist nurse) opens the patient's mouth, inserts the laryngoscope to the right of the mouth, moves the tongue to the left, pushes the light deep, coordinates With the right hand, press down on the cricoid cartilage to find the epiglottis and glottis. Perform rapid induction of anesthesia and the Sellick maneuver in case of full stomach. Gently insert the endotracheal tube through the glottis, stopping when the balloon of the endotracheal tube passes 2-3 cm through the vocal cords. Remove the laryngoscope, then inflate the endotracheal balloon. To check that the endotracheal tube is in the correct position, the doctor will listen to the lungs and EtCO2 results. If it is in place, the doctor will secure the tube with tape and place the cannula in the mouth to prevent biting if necessary.

Kỹ thuật đặt nội khí quản qua đường miệng
Technique of nasal intubation
The doctor chooses the side of the nose that will intubate the trachea, instilling vasoconstrictor drugs such as naphazoline, otrivine, ... into the nose. Then select an endotracheal tube of appropriate size, insert the endotracheal tube lubricated with lidocaine grease through the nostril. Open the patient's mouth, insert the laryngoscope to the right of the mouth, slide the patient's tongue to the left, push the lamp deep, and coordinate with the right hand to press the cricoid cartilage to find the epiglottis and glottis. In favorable cases, proceed to gently insert the endotracheal tube through the glottis, stopping when the balloon of the endotracheal tube passes 2-3cm through the vocal cords. In difficult cases, use Magill pliers to guide the tip of the endotracheal tube into the correct glottis, the assistant pushes the endotracheal tube from the outside. Gently withdraw the laryngoscope, then inflate the endotracheal balloon. The doctor checks that the endotracheal tube is in the correct position by listening to the lungs and checking the EtCO2 results. Secure the endotracheal tube with adhesive tape. In case of unsuccessful implementation of the above two procedures, the anesthesia team will switch to performing the difficult intubation procedure.
To maintain anesthesia when the surgery takes place, the patient will be used intravenous or volatile anesthetics, pain relievers, muscle relaxants (if needed). The depth of anesthesia will be closely monitored based on parameters such as heart rate, blood pressure, sweating, tearing (PRST); MAC, BIS, Entropy (if any). The patient's breathing is controlled by machine or hand squeeze. In addition, must always closely monitor vital signs and prevent the endotracheal tube from being misplaced, flexed, or blocked.

Để duy trì mê khi cuộc mổ diễn ra, người bệnh sẽ được sử dụng thuốc mê tĩnh mạch
2.4. Criteria for extubation
After surgery to correct kyphoscoliosis is completed, the endotracheal tube is removed when the patient meets the following criteria:
Patient is awake, can follow orders, lifts his head more than 5 pages, TOF > 0.9 Self-breathes Regular, breathing rate within normal limits, stable blood pressure, body temperature > 35 degrees Celsius, no complications of anesthesia and surgery.
3. Complications that may occur during endotracheal anesthesia surgery to correct kyphosis scoliosis
3.1. Reflux of gastric juice into airway
When detecting that the patient has digestive juices in the oral cavity and airways, the anesthesiologist team immediately aspirates the fluid, has the patient lie down with his head low, and tilts his head to the side. Place the endotracheal tube quickly and clear the airway. Closely monitor the patient after surgery to prevent lung infection.
3.2. Hemodynamic disorders
During endotracheal anesthesia for kyphosis scoliosis surgery, patients may experience hemodynamic disturbances such as hypertension, hypotension, and cardiac arrhythmias. The doctor will treat according to the specific symptoms and causes of each patient.

Rối loạn nhịp tim là một tai biến có thể gặp khi gây mê nội khí quản phẫu thuật chỉnh gù vẹo cột sống
3.3. Complications due to endotracheal intubation
Many complications can occur during intubation for anesthesia such as:
Failure to intubate: If this is the case, the doctor will switch to a difficult intubation procedure or switch to another method of insensitivity. Misplaced in the stomach: If there is no alveolar murmur on auscultation, EtCO2 cannot be measured, it is possible that the endotracheal tube was mistakenly placed in the stomach. The doctor will reposition the endotracheal tube. Vocal-tracheal-bronchospasm: If it is difficult or impossible to ventilate the patient, auscultates the lungs with rales or mutes the lungs, the anesthesiology team will provide adequate oxygen, add sleeping pills and relax muscles, to ensure ventilation and give bronchodilators, corticosteroids. If breathing is still not controlled, move on to a difficult intubation procedure. Trauma during endotracheal intubation: Injuries that may occur during intubation such as bleeding, tooth fracture, vocal cord injury, foreign object fall into the airway,... Treatment of injuries damage on a case-by-case basis.
3.4. Respiratory complications
Hypoxia and anthrax will occur if the endotracheal tube is folded, retracted, pushed deep into one lung, collapsed or opened the respiratory system, the oxygen source is exhausted, the soda is ineffective,... Anesthesia will immediately ensure ventilation, provide 100% oxygen and treat the cause.

Khi người bệnh thiếu oxy trong quá trình gây mê cần đảm bảo ngay thông khí, cung cấp oxy 100%
3.5. Complications after extubation
After extubation, patients may experience complications such as respiratory failure, sore throat, hoarseness, laryngotracheal spasm, upper respiratory tract infection, laryngotracheal stenosis,. .. The doctor will treat according to the symptoms and causes.
Endotracheal anesthesia is a routine anesthetic technique performed at Vinmec International General Hospital. Accordingly, the procedure of endotracheal anesthesia at Vinmec is carried out methodically and in accordance with standard procedures by a team of highly skilled doctors and modern machinery. As a result, complications after anesthesia and surgery are always minimized to the maximum extent.
Doctor Quoc Tuan has many years of experience in the field of Anesthesiology - resuscitation at Hoan My Danang Hospital and Phu Yen Provincial General Hospital before being an Anesthesiologist and resuscitator at the Operating Room - Department of Medicine. General surgery of Vinmec Nha Trang International General Hospital as it is today.
If you have a need for medical examination by modern and highly effective methods at Vinmec, please register here.