This is an automatically translated article.
The article was professionally consulted by Specialist Doctor I Ho Quoc Tuan - Anesthesiologist - General Surgery Department - Vinmec Nha Trang International General Hospital.Endotracheal anesthesia is a method of general anesthesia with endotracheal intubation to help control breathing in head and neck abscess surgery and postoperative resuscitation. Accordingly, to limit complications, patients need to follow the doctor's instructions and orders.
1. Abscess surgery in the head, face and neck area
Head and neck abscesses include many types such as submandibular abscess, lateral wall abscess, cheek abscess, neck abscess, etc. There are many common causes of head and neck abscesses. It is caused by oral infections, salivary gland infections, complications of wisdom teeth, trauma or infection of the surrounding areas. Patients with abscesses in the head, face and neck often have signs of infection such as high fever, chills, rapid pulse, tachycardia, headache, trouble sleeping, dry lips, dirty tongue... Abscess mass is a Massive swelling, the skin over the abscess is swollen, red, hot, red or purple, tight, swollen, may infiltrate and spread to the surrounding areas, intense pain to the touch.
If not treated promptly and properly, abscesses in the head, face and neck will lead to many dangerous complications such as diffuse inflammation of the face, respiratory paralysis due to acute laryngitis, purulent meningitis, and infection. Blood pressure, septic shock ... The principle of treating abscesses in the head, face and neck area is to surgically reveal the abscess, remove all lesions, effectively drain, fight infection and support the body.
Endotracheal anesthesia is one of the anesthetic methods used in head and neck abscess surgery. Endotracheal anesthesia is a difficult technique, so the technique is not performed if the patient does not agree or the medical facility does not have enough facilities for anesthesia and resuscitation, or medical staff are not proficient in the technique.
Áp xe vùng đầu mặt cổ có thể gây nhiễm trùng huyết khi không được điều trị sớm
2. Preparation for endotracheal anesthesia for head and neck abscess surgery
The person performing the technique of endotracheal anesthesia for head, face and neck abscess surgery is a doctor, a nurse specializing in anesthesiology and resuscitation. Necessary facilities to perform endotracheal anesthesia include:
Anesthesia machine with breathing system, vital function monitor (ECG indicators, arterial blood pressure, SpO2, EtCO2, breathing rate, temperature) degree), hand squeeze oxygen source, defibrillator, suction machine,...; Laryngoscope, endotracheal tube of various sizes, suction tube, mask, squeeze balloon, oropharyngeal cannula, Magill pliers, soft mandrin; Lidocaine 10% spray, Salbutamol spray; Means to prevent difficult intubation: Cook tube, laryngeal mask, flexible bronchoscope, tracheostomy kit, mouth opener,... Before performing surgery, the doctor will examine anesthesia. , assessment, detection and prevention of possible risks. The patient will be explained the purpose and procedure to cooperate with the doctor. In case of need, the patient will be prescribed a sedative by the doctor from the night before the surgery.

Bệnh nhân có thể sử dụng thuốc an thần trước khi phẫu thuật
3. Procedure of endotracheal anesthesia for head, face and neck abscess surgery
3.1. Steps to conduct endotracheal anesthesia for head and neck abscess surgery
After checking the records and examining the patient, the anesthesia team will have the patient lie on his back on the operating table, breathe 100% oxygen with a flow rate of 3-6 liters/minute at least 5 minutes before the induction of anesthesia. Install the monitor, set up the line and pre-anesthesia (if necessary).
Perform induction of anesthesia with drugs:
Sleeping pills: you can use anesthetic drugs such as intravenous anesthetics (propofol, etomidate, thiopental, ketamine,...), volatile anesthetics (sevoflurane, Isoflurane, etc.). ..) Painkillers: fentanyl, sufentanil, morphine,... Muscle relaxants: rocuronium, succinylcholine, vecuronium,... are used if necessary. The condition for intubation is that the patient sleeps deeply and has enough muscle relaxation (in most cases). There are two techniques that can be used for endotracheal intubation: oral intubation and nasal intubation.

Bệnh nhân được gây mê tĩnh mạch trước khi phẫu thuật
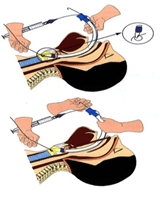
Oral intubation technique
The doctor (or anesthesiology specialist nurse) opens the patient's mouth, inserts the laryngoscope to the right of the mouth, moves the tongue to the left, pushes the light deep, coordinates With the right hand, press down on the cricoid cartilage to find the epiglottis and glottis. Perform rapid induction of anesthesia and Sellick procedure in case of full stomach (pressing the cricoid cartilage 20-30 kg as soon as the patient loses consciousness until the intubation is complete). Pass the endotracheal tube gently through the glottis, stopping when the balloon of the endotracheal tube passes 2-3 cm through the vocal cords. Remove the laryngoscope, then inflate the endotracheal balloon. The doctor will listen to the lungs and EtCO2 results to check that the endotracheal tube is in the correct position. If it is in the correct position, the doctor will secure the tube with tape and place the cannula in the mouth to prevent biting the tube (if necessary). Nasal intubation technique
The doctor chooses the side of the nose that will intubate the trachea, instilling vasoconstrictor drugs such as naphazoline, xylometazoline... into the nose. Then select an endotracheal tube of appropriate size, insert the endotracheal tube lubricated with lidocaine grease through the nostril. Open the patient's mouth, insert the laryngoscope to the right of the mouth, slide the patient's tongue to the left, push the lamp deep, and coordinate with the right hand to press the cricoid cartilage to find the epiglottis and glottis. In favorable cases, proceed to gently insert the endotracheal tube through the glottis, stopping when the balloon of the endotracheal tube passes 2-3cm through the vocal cords. If it is difficult, use Magill pliers to guide the tip of the endotracheal tube into the correct glottis, the assistant pushes the endotracheal tube from the outside. Gently withdraw the laryngoscope, then inflate the endotracheal balloon. The doctor checks that the endotracheal tube is in the correct position by listening to the lungs and checking the EtCO2 results. Secure the endotracheal tube with adhesive tape.

Kỹ thuật đặt nội khí quản qua đường miệng
In case of unsuccessful implementation of the above two procedures, the team will apply the difficult endotracheal intubation procedure.
To maintain anesthesia during surgery, the patient will be given intravenous or volatile anesthetics, pain relievers and muscle relaxants (if needed). Respiration is controlled by machine or hand squeeze. The depth of anesthesia will be closely monitored based on parameters such as heart rate, blood pressure, sweating, tearing (PRST); MAC, BIS, Entropy (if any).
3.2. Criteria for extubation
After surgery for head, face and neck abscess is over, the endotracheal tube is removed when the patient meets the following criteria:
The patient is awake, can follow orders, breathes spontaneously, and the respiratory rate is within normal limits. often. Self-elevating head over 5 seconds, TOF >0.9, stable blood pressure, body temperature >35 degrees Celsius, no complications of anesthesia and surgery.
4. Possible complications during endotracheal anesthesia and scoliosis correction surgery
4.1. Reflux of gastric juice into airway
If the patient has digestive juices in the oral cavity and airway, the anesthesiologist team immediately drains the fluid, has the patient lie down with his head low, and tilts his head to the side. Promptly intubate the endotracheal tube and clear the airway. Patients will be closely monitored after surgery to prevent lung infections.
Trào ngược dịch dạ dày vào đường thở là một tai biến sau phẫu thuật
4.2. Hemodynamic disorders
The hemodynamic disturbances that may be encountered during endotracheal anesthesia for head and neck abscess surgery are hypertension, hypotension, and cardiac arrhythmias. The doctor will treat according to the specific symptoms and causes of each patient.
4.3. Complications due to endotracheal intubation
Many complications can occur during intubation such as:
Failed to intubate: the solution is to switch to difficult intubation procedure or switch to another method of anesthesia. Misplaced in the stomach: The endotracheal tube was mistakenly placed in the stomach when listening to the lungs without alveolar murmur, EtCO2 could not be measured. The doctor will reposition the endotracheal tube. Vocal-tracheal-bronchospasm: When it is difficult or impossible to ventilate the patient, auscultates the lungs with rales or mutes the lungs, the anesthesiology team will handle it by providing adequate oxygen, adding sleeping pills and relaxing muscles, ensure ventilation and give bronchodilators, corticosteroids. Switch to a difficult intubation procedure if breathing is still not controlled. In addition, some injuries may occur during intubation such as bleeding, tooth fracture, vocal cord damage, foreign object falling into the airway,... Injuries will be handled on a case-by-case basis. specific situations.
4.4. Respiratory complications
If the endotracheal tube is folded, retracted, pushed deep into one lung, collapsed or opened the respiratory system, the oxygen source is exhausted, the soda is ineffective, ... will lead to hypoxia and hypercapnia. Anesthesia team will immediately ensure ventilation, provide 100% oxygen and treat the cause.

Bệnh nhân được cung cấp oxy 100% khi hết nguồn oxy
4.5. Complications after extubation
After extubation, the patient may experience complications such as respiratory failure, sore throat hoarseness, laryngotracheal spasm, upper respiratory tract infection, laryngotracheal stenosis, .. The doctor will handle each case on a case-by-case basis.
Endotracheal anesthesia is a routine anesthetic technique performed at Vinmec International General Hospital. Accordingly, the procedure of endotracheal anesthesia at Vinmec is carried out methodically and in accordance with standard procedures by a team of highly skilled doctors and modern machinery. As a result, complications after anesthesia and surgery are always minimized to the maximum extent.
Doctor Quoc Tuan has many years of experience in the field of Anesthesiology - resuscitation at Hoan My Danang Hospital and Phu Yen Provincial General Hospital before being an Anesthesiologist and resuscitator at the Operating Room - Department of Medicine. General surgery of Vinmec Nha Trang International General Hospital as it is today.
If you have a need for medical examination by modern and highly effective methods at Vinmec, please register here.