This is an automatically translated article.
Posted by Master, Doctor Mai Vien Phuong - Department of Examination & Internal Medicine - Vinmec Central Park International General Hospital
Recent advances in endoscopic technology allow detailed visualization of the gastric mucosa. Today, endoscopy is used in the diagnosis of gastritis to determine the presence/absence of Helicobacter pylori (H. pylori) infection and to assess gastric cancer risk. In 2013, the Japan Society of Gastroenterology Endorsed the Kyoto Classification, a new classification system for endoscopic gastritis.
The Kyoto classification provided endoscopic findings associated with H. pylori infection. The Kyoto classification score is the sum of five endoscopic findings (atrophy, intestinal metaplasia, hypertrophic folds, nodules, and diffuse redness with or without regular arrangement of the RAC collection venules) and ranges from 0 to 8.
1. Atrophy, intestinal metaplasia, hypertrophic folds and nodules contribute to gastric cancer risk
Diffuse redness and regular arrangement of venules are associated with H. pylori infection. In subjects with no history of H. pylori eradication, the infection rates in those with a Kyoto score of 0, 1 and ≥ 2 were 1.5%, 45%, and 82%, respectively. The Kyoto classification score of 0 indicates no H. pylori infection. A Kyoto classification score of 2 or higher indicates H.pylori infection. The Kyoto classification scores of patients with and without gastric cancer were 4.8 and 3.8, respectively. A Kyoto classification score of 4 or higher may indicate an increased risk of stomach cancer.
2. Endoscopic evaluation findings of the Kyoto classification
Kyoto classification of endoscopic findings based on Helicobacter pylori (H. pylori) infection. The Kyoto classification score is the sum of the five endoscopic findings (atrophy, intestinal metaplasia, hypertrophy of mucosal folds, nodules, and diffuse redness with or without regular arrangement of the collecting venules). ) and ranges from 0 to 8. A high score is thought to reflect a higher risk of current H. pylori infection and stomach cancer. The Kyoto classification score of 0 indicates no H. pylori infection. The Kyoto classification score ≥ 2 indicates current H. pylori infection. A Kyoto classification score of ≥ 4 may indicate an increased risk of gastric cancer.
Nhiễm vi khuẩn H.pylori gây ung thư dạ dày
3. Stomach cancer and H. pylori infection - the main cause of stomach cancer
Stomach cancer is the third most common cancer in the world and the cancer with the third largest number of deaths. If stomach cancer is detected at an early stage, it can be cured through endoscopic submucosal dissection. Although routine endoscopy is important for early detection of gastric cancer, effective surveillance requires identification of high-risk populations. Inherited risk factors for gastric cancer have been reported to include hereditary cancer syndromes, single nucleotide polymorphisms, and family history. Environmental risks include Helicobacter pylori infection, smoking, eating too much salt, and lack of vegetables. Among them, an association between H. pylori infection and the development of gastric cancer has been well established, and H. pylori virulence factors (cagA, vacA, iceA, and DupA) have been established. known.
The International Agency for Research on Cancer has classified H. pylori infection as a class I carcinogen and it is considered a major cause of stomach cancer. On the other hand, eradication of H. pylori reduces the risk of stomach cancer. Therefore, accurate assessment of H. pylori infection is important. Today, endoscopic examination is required to diagnose H. pylori infection. In 2013, the Japan Society of Gastroenterology Endorsed the Kyoto Classification, a new classification system for endoscopic gastritis. In this review, the authors focus on updated reports related to the Kyoto classification to help improve endoscopic practice.
4. Kyoto classification definition of gastritis
Thanks to advances in endoscopic technology, it is now possible to observe the gastric mucosa in minute detail. Today, endoscopy is used in the diagnosis of gastritis to determine the presence/absence of H. pylori infection and to assess gastric cancer risk. The Kyoto classification of endoscopic findings was advocated when the 85th Meeting of the Japanese Society of Gastroenteroscopy was held in Kyoto in 2013. The purpose of the Kyoto classification was to evaluate the list of endoscopic findings. gastric mucosa, as this carries a potential risk of developing stomach cancer. In this classification, 19 endoscopic findings associated with gastritis, including atrophy, intestinal metaplasia, hypertrophic folds (elbow folds), nodules, diffuse redness, and regular arrangement of the urinary bladder collection vein (RAC), map red, gastric hyperplastic polyp, xanthoma, characterized by mucosal edema, patchy red, mucosal indentation, sticky mucus, blood clots, red streaks, mottled red mottled, numerous white and flat lesions, basal adenomatous polyps, and elevated erosions. Among them, atrophy, intestinal metaplasia, hypertrophic mucosal folds and nodules, which may be associated with gastric cancer risk, and diffuse erythema with or without RAC, are associated with H. pylori, included in the Kyoto classification score Endoscopic mucosal atrophy (Kimura-Takemoto classification):
Atrophy includes “pathological” and “endoscopic” atrophy. Atrophy is defined pathologically as loss of glandular tissue. Kyoto classification through Kimura-Takemoto classification of endoscopic atrophy. Kimura et al identified a visible, low reflective, and pale yellow capillary network as characteristic of atrophy, while diffuse redness with high mucosal height was characteristic of nonatrophy. “endoscopic” atrophy has been reported to correlate well with “pathological” atrophy. In the Kyoto classification, non-atrophy (C0) and C1 are said to be atrophy 0, C2 and C3 are atrophy 1, and O1 to O3 are atrophy 2.
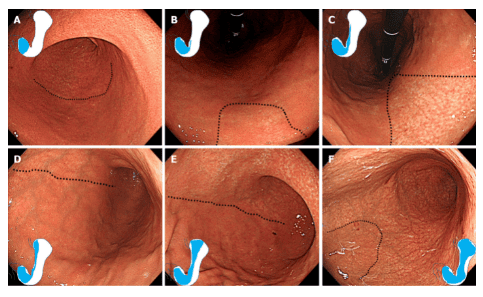
Kimura-Takemoto phân loại teo nội soi. Đường viền teo được biểu thị bằng một đường chấm. A: C1 (Teo chỉ giới hạn ở hang vị); B: C2 (Teo chỉ giới hạn ở vùng nhỏ của bò cong nhỏ); C: C3 (Teo tồn tại chủ yếu ở góc bò cong nhỏ nhưng không lan đến tâm vị); D: O1 (Teo kéo dài đến tâm vị. Đường viền của vùng teo nằm giữa bờ cong nhỏ hơn và thành trước dạ dày); E: O2 (Đường viền teo thân vị nằm ở thành trước); F: O3 (Teo lan rộng với ranh giới giữa thành trước và bờ cong lớn dạ dày).
Intestinal metaplasia on endoscopic:
Intestinal metaplasia usually presents as grayish-white and slightly elevated patches surrounded by areas of pale pink and mixed patchy mucosa, forming an uneven surface. Villi-like appearance, whitish mucosa, and rough mucosal surface are useful markers for endoscopic diagnosis of intestinal metaplasia. Advanced imaging endoscopy, including narrow band imaging (NBI), blue laser imaging, and associated color imaging, has improved the visibility of endoscopic findings and the accuracy of endoscopic diagnosis intestinal metaplasia. Opaque patches on the superficial epithelium and pale green on the rim of the mucosal epithelium visualized by magnified NBI are associated with intestinal metaplasia
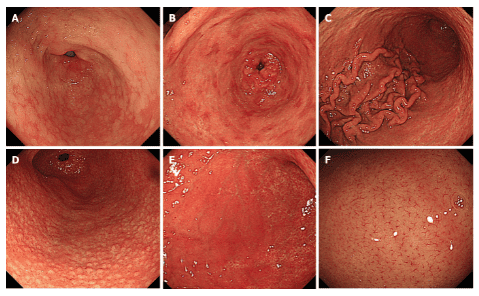
Kết quả nội soi về phân loại Kyoto. A: Viêm chuyển sản ruột; B: Đỏ như bản đồ; C: Các nếp gấp phì đại ; D: Tổn thương dạng nốt; E: Đỏ da lan tỏa; F: Sự sắp xếp đều đặn của các tiểu tĩnh mạch RAC trong hình ảnh được phóng đại thấp
In the Kyoto classification, the absence of intestinal metaplasia is said to be zero of intestinal metaplasia, the presence of intestinal metaplasia in the antrum is the point of intestinal metaplasia 1, and intestinal metaplasia extending into the body is Intestinal metaplasia score 2. Intestinal metaplasia score is diagnosed using white light imaging. Advanced endoscopy-based diagnosis of intestinal metaplasia using the NBI regimen, blue laser imaging, associated color imaging, and staining endoscopy were not included in the Kyoto score. The atlas red mucosal image (synonymous with irregular congestive lesions of the mucosa) is defined as multiple flat or slightly concave red lesions of varying shape, size, and red density. When using red-colored biopsies as atlas, intestinal metaplasia is commonly observed (87.3%). The mechanism of the map-like appearance of red is thought to enhance the contrast between atrophic and non-atrophic mucosa after diffuse redness has disappeared after successful eradication of H.pylori. Map red is not always found after eradication of H.pylori. However, when it is observed, there is almost no doubt that it is a sign of mucosa that has been treated with eradication of H.pylori. Hypertrophic folds:
A hypertrophic fold is defined as a fold 5 mm or more in width that is not flattened or only partially flattened by stomach contractions. Rugal hyperplasia is a synonym for hypertrophy of mucosal folds. In the Kyoto classification, the absence and presence of hypertrophic folds are scored, with hypertrophic folds 0 and 1 respectively.
Nodularity:
Gastritis Nodular thickening is characterized by a millet-like “goose skin” pattern mainly located in the antrum. The roughness can be seen more clearly after the application of Indigo carmine dye. Lymphatic cysts and/or excessive inflammatory cell infiltration were observed in these nodular biopsies. Nodular gastritis manifests mainly in women and improves with age. High serum H. pylori antibody titer correlates with nodularity. In the Kyoto classification score, the absence and presence of nodules are scored as Nodularity scores 0 and 1, respectively.
Diffuse red:
Diffuse red refers to a uniform red with continuous dilation being concerned. Non-atrophic mucosa is observed mainly in the body and is typical of endoscopic superficial gastritis. Obstruction and dilation of the subepithelial capillary network in the gastric mucosa with inflammation changes the mucosal surface color to red. Because the assessment of the extent of diffuse conjunctivitis of the antrum is affected by the placement of the endoscope and monitor, objective assessment can be difficult. On the other hand, RAC is a condition in which the collecting venules are arranged in the corpus. From a distance, it looks like an infinite number of dots. Seen from up close, it looks like a regular starfish. In the Kyoto grading scale, cases where diffuse red is absent are scored as diffuse red 0, mildly diffuse red, or diffuse red with RAC of diffuse red 1 and severely diffuse red or diffuse red no. RAC is Diffuse Red 2.
5. Kyoto Classification Score
The Kyoto gastritis classification score is based on the total score of five endoscopic findings and ranges from 0 to 8. A high score is thought to reflect an increased risk of H. pylori infection and gastric cancer.
The Kyoto classification provided endoscopic findings associated with H. pylori infection. Kyoto classification score ≥ 2 indicates H. pylori infection. Testing for H. pylori is essential in cases where there is no history of H. pylori eradication therapy. A Kyoto classification score of ≥ 4 may indicate an increased risk of gastric cancer. Such cases need careful monitoring. However, research regarding the Kyoto score is still scant and more research is needed.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.