This is an automatically translated article.
The article was professionally consulted by Specialist Doctor I Tran Quoc Vinh - Emergency Doctor - Department of Resuscitation - Emergency - Vinmec Nha Trang International General Hospital.Pericarditis is defined as inflammation of the pericardium, the disease is usually self-limited and benign. However, empyema in children is a serious condition and has a high mortality rate. Therefore, the goal is to detect this disease early and take active measures to control the infection, avoiding its spread and endangering the child's life.
1. What is empyema in children?
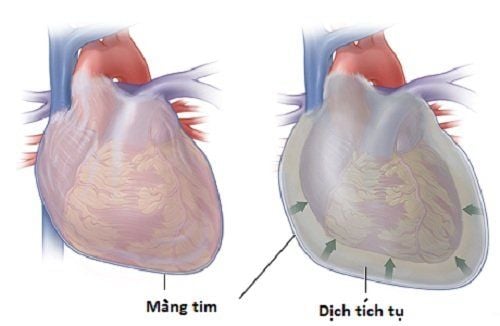
Empyema pericarditis is a disease that is generally quite rare in childhood. This is a condition associated with bacterial inflammation of the pericardium and the presence of pus in the pericardial cavity. Once acquired, the disease is often severe and, in some cases, still potentially life-threatening even after antibiotic use has become widespread.
Different from common pericarditis cases which can be caused by bacteria, fungi and viruses, pyelonephritis in children is mainly caused by bacterial agents and the purulent inflammatory process sometimes takes place. at a fast rate, creating a lot of fluid, causing cardiac tamponade. Awareness of this pathology has increased today due to the advent of non-invasive diagnostic techniques, such as echocardiography, computed tomography (CT) and cardiac magnetic resonance imaging (CMRI). However, the outcome of the disease has not improved significantly, especially in children with immunosuppression or infections affecting the myocardium causing myocarditis.
Viêm mủ màng tim ở trẻ em do tác nhân vi khuẩn gây ra
2. What are the symptoms of children with empyema?
Most children with empyema have a severe presentation and sometimes have symptoms that suggest sepsis in the first place. Furthermore, acute empyema in the newborn is a medical emergency; Therefore, prompt assessment, diagnosis and treatment are essential.
Symptoms in children with empyema are often nonspecific and may be similar to common infections, including fever, tachypnea, and tachycardia according to the degree of fever. Older children may complain of an upset stomach. Primary chest pain is not a common symptom, especially in young children. If present in older children, they may describe a sharp or dull pain. The supine position, chest wall movements such as forceful coughing can aggravate the pain, but sitting forward can reduce the pain. In case of a lot of pus overflow, it can lower blood pressure and cause cardiogenic shock due to compression.
In addition, empyema is also a complication of infectious diseases of neighboring organs, so the child is hospitalized because of symptoms of these organ systems such as:
Pneumonia Meningitis Osteomyelitis Acute myelitis Acute arthritis Soft tissue infection Neonatal infection

Trẻ xuất hiện triệu chứng sốt
For infants with pericarditis, the general condition of the child is often very ill, possibly due to premature birth, low birth weight and signs of severe sepsis or shock with manifestations such as lethargy, sleep chicken, quit suckling. At the same time, this diagnosis should be suspected in any infant who both appears to have sepsis and has an abnormal cardiovascular examination with a very rapid heart rate. This is an indicator of both purulent pericarditis and acute myocarditis.
On examination, the classic sign of pericarditis is pericardial rubbing. This finding is not specific for the fluid nature of the pericardial cavity; however, if the volume is large, the rubbing becomes hard to hear and the baby's heart sounds become fainter.
In addition, other signs may also be seen in empyema in children similar to symptoms of right heart failure in adults with distended jugular veins, hepatomegaly and leg edema, ascites. However, these signs can be difficult to assess in young children, especially infants.
In the case of a large amount of pericardial effusion, the child will have symptoms of hypotension, dyspnea, paradoxical pulse, heart failure with low cardiac output and circulatory collapse. At this time, if not treated in time, it can be life-threatening.
3. What tests should be done in children with empyema?
In addition to the above signs, sometimes non-specific, the diagnosis of pyelonephritis in children must also rely on blood tests, pericardial fluid tests, electrocardiograms and imaging facilities. such as X-ray, echocardiography or computed tomography (CT), cardiac magnetic resonance imaging (MRI).
3.1. Blood test A complete blood count is a prerequisite test to be performed. In the case of bacterial empyema, the white blood cell count will be elevated with the predominance of immature polymorphonuclear leukocytes.
Blood cultures should also be performed to help confirm or rule out the possibility of sepsis. It has been reported that positive blood cultures occur in more than half of children with bacterial pericarditis. In addition, the erythrocyte sedimentation rate, acute inflammatory phase reactants such as C-reactive protein (CRP) are also increased and Pro-calcitonin is increased (increased in bacterial infection) in purulent pericarditis.
In addition, increased levels of troponin T and troponin I have been reported in children with pericarditis, troponin T, I are components in cardiomyocytes, and troponin T, I are increased in myocardial injury. This may indicate co-occurrence of latent myocarditis and a more severe prognosis than in cases without troponin elevation.

Xét nghiệm máu ở bệnh viêm mủ màng tim ở trẻ em
3.3. Electrocardiogram Most patients present with at least one ECG abnormality, the most common being sinus tachycardia, voltage staggered, and ST-segment changes. pericardial effusion, PR depression is indicative of pericarditis, while saddle-shaped ST elevation in most leads except aVR, V1 (possible ST depression) is indicative of myositis heart. However, these markers are not very sensitive.
3.4. Imaging facilities Chest X-ray: This is the first imaging needed to help preliminary assessment of damage not only of the heart but also of the lung parenchyma. If pericardial effusion is present, the heart shadow will be enlarged, as assessed by a cardiothoracic index > 1/2. Echocardiography: This is the imaging modality of choice to quickly and accurately identify pericardial effusion as well as determine the volume of fluid, the risk of cardiac tamponade. However, the limitation of this imaging modality, as well as chest X-ray, is that it does not reveal the nature of fluid in the pericardial cavity. However, ultrasonography will be essential to determine the site of puncture if the volume is very small or the effusion is localized. CT and MRI: Compared with the above two techniques, CT and MRI can help confirm the thickness of the pericardial effusion, evaluate pericardial thickening, and also help identify other abnormalities, such as lymph nodes. blood in the mediastinum, helping to pinpoint the cause more precisely. Not only that, but cardiac MRI showed early lesions of coexisting myocarditis.

Siêu âm tim được thực hiện giúp chẩn đoán bệnh
4. How to treat empyema in children?
The treatment of empyema in children is similar to that in adults. In particular, the components of treatment include the use of antibiotics in full regimens and surgical procedures on the pericardium.
4.1. Antibiotics Systemic antibiotic therapy must be initiated early, as soon as the diagnosis is established and even when results of microbiological cultures are not available. The antibiotic of choice initially is usually empiric local antibacterial spectrum such as vancomycin, ceftriaxone or imipenem, meropenem or piperacillin-tazobactam plus fluconazole if the disease occurs in the child with a predisposed immunocompromise.
Because of the limited permeability to the pericardial cavity, antibiotic therapy should be maintained for at least 28 days or until the child is fever-free and there are no signs of infection on blood tests.

Kháng sinh được sử dụng trong điều trị viêm mủ màng tim ở trẻ em
4.2. Surgical intervention These techniques will be considered depending on the acquired disease, the patient's condition as well as the availability of necessary facilities and the skill of the surgeon. Accordingly, common surgical procedures to remove pus in the pericardial cavity include local aspiration or drainage of the pericardium, opening a "window" on the pericardium, or surgical removal of the pericardium.
Regardless of the method chosen, the goal to be achieved is to completely resolve the pus-filled cavity, avoid the infection from spreading to the whole body as well as prevent complications of constrictive pericarditis later for the child.
In summary, although it is quite rare, empyema in children is quite severe and has a high risk of death. Once confirmed, antibiotic treatment should be initiated immediately; and consider early surgical intervention when the patient's general condition allows. Only by doing so can the child's prognosis become better and the long-term complications will be reduced.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.