This is an automatically translated article.
Tuberculosis and Chronic Obstructive Pulmonary Disease (COPD) are both diseases with many similarities that can cause confusion. In order to make an accurate diagnosis and get the right treatment, the patient should know the basic information and how to distinguish between the two diseases.
1. Causes of pulmonary tuberculosis
Pulmonary tuberculosis is a disease of the lungs caused by tuberculosis bacteria, which can be spread from person to person mainly through the respiratory tract. If a person with pulmonary tuberculosis is tested for bacteria in their sputum, when talking or sneezing, they will accidentally release a large amount of TB bacteria into the environment, causing infection to others. Other contacts such as shaking hands, touching... do not spread TB.
Pulmonary tuberculosis usually has a subacute presentation (that is, it does not progress as acutely as bronchitis and pneumonia, but it does not have to be long-lasting, such as COPD, diabetes, heart failure, etc.).
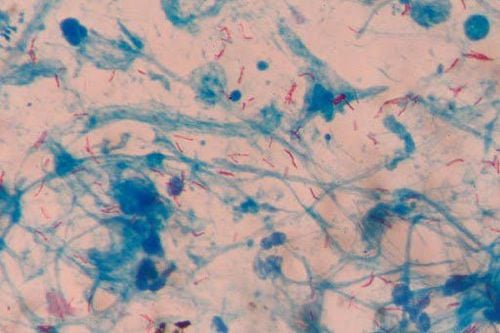
Hình ảnh vi khuẩn lao phổi
2. Causes of Chronic Obstructive Pulmonary Disease (COPD)
If pulmonary tuberculosis is a disease with subacute manifestations (that is, it is not acute like pneumonia, bronchitis, but it is also not long-term chronic such as diabetes, heart failure ..) Chronic Obstructive Pulmonary Disease (COPD) is a chronic disease caused mainly by tobacco, pipe tobacco and environmental factors.
Unlike tuberculosis, COPD is not caused by bacteria, so it is not spread from person to person. However, if a group of people are exposed to the same risk factors (such as cigarette smoke or polluted environments), they can show similar symptoms.
80-90% of people with chronic obstructive pulmonary disease (COPD) are tobacco-related, but only 15-20% of smokers have COPD. Research shows that the more "sensitive" people are to secondhand smoke, the more likely they are to become seriously ill.
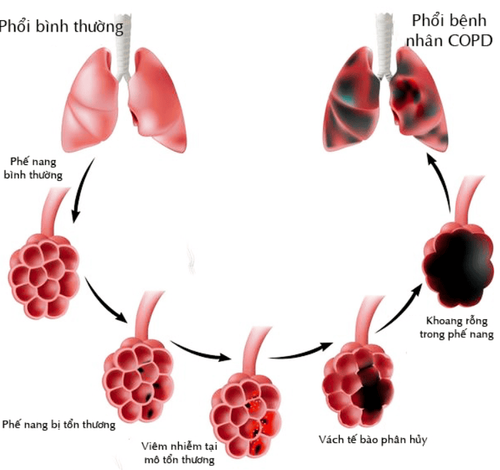
Bệnh phổi tắc nghẽn mạn tính COPD
Trắc nghiệm: Làm thế nào để có một lá phổi khỏe mạnh?
Để nhận biết phổi của bạn có thật sự khỏe mạnh hay không và làm cách nào để có một lá phổi khỏe mạnh, bạn có thể thực hiện bài trắc nghiệm sau đây.3. Distinguishing symptoms
Symptoms of chronic obstructive pulmonary disease (COPD) are cough, sputum production, and shortness of breath on exertion and tend to increase.
Persistent or intermittent cough: Due to the nature of the chronic disease, COPD causes a cough that lasts for at least 3 months in 1 year, dry cough or sputum. This is also a common symptom and is difficult to see in other lung diseases such as bronchiectasis, pulmonary tuberculosis... Shortness of breath: The patient will feel shortness of breath gradually over time, at first it is shortness of breath with exertion. after shortness of breath even at rest and continuous shortness of breath. Patients must struggle to breathe, have a feeling of lack of air or heavy breathing, wheezing, gasping. Over time, the symptoms of persistent cough, sputum production, and shortness of breath will get worse over time. Usually, the signs of cough and sputum appear first, then the symptoms of shortness of breath appear, when the patient has difficulty breathing, that is when the patient has entered the severe stage.
Pulmonary tuberculosis often presents with general symptoms of TB syndrome such as fatigue, loss of appetite, weight loss, low-grade fever or chills, night sweats at night, accompanied by pulmonary symptoms such as cough , spitting up sputum, sometimes coughing up blood.
The best way to detect pulmonary TB is that you need to go to the hospital for TB screening if you see the following signs:
Cough, producing sputum that lasts for 3 weeks or more Coughing up blood Chest pain or pain when breathing or coughing Fatigue, anorexia, exhaustion, unintended weight loss

Người bệnh cảm thấy đau ngực
4. Diagnostic measures
To diagnose pulmonary tuberculosis, doctors will combine information from the source of infection, clinical signs, chest X-ray and some other tests such as tuberculous response (IDR), bacteria tuberculosis (BK, AFB) in the sputum, assess the density of lymphocytes in the blood, erythrocyte sedimentation rate (VS)...
If the chest X-ray results show unilateral or bilateral infiltrates or the lungs are seen Perforation forming tubercles is also a sign that the patient has pulmonary tuberculosis.
For chronic obstructive pulmonary disease (COPD), the doctor will diagnose based on the patient's history of exposure to risk factors, clinical manifestations such as dry cough and shortness of breath are all signs of airway obstruction. The airway is not fully restored.
Because pulmonary tuberculosis and chronic obstructive pulmonary disease (COPD) both have respiratory symptoms such as cough, sputum production, there may be shortness of breath, difficulty in breathing, so it is sometimes easy to confuse these two diseases. Therefore, to make an accurate diagnosis, your doctor will often order some additional tests as outlined above.

Xét nghiệm tìm vi trùng lao (BK, AFB) trong đờm
5. Treatment measures
5.1 Treatment of pulmonary tuberculosis The treatment for tuberculosis includes improving fitness and using anti-tuberculosis drugs. Antituberculosis drugs are antimicrobial drugs that can be mentioned: Streptomycin (injection) and 4 drugs taken orally: Rifampicin, Isoniazid, Ethambutol and Pyrazinamide. The duration of treatment for pulmonary tuberculosis will last about 6 to 8 months. If the patient is detected and treated early and adheres to the correct treatment regimen, after the above time, the disease will be completely cured and leave no sequelae. However, if the treatment is delayed or not followed properly, it will leave many sequelae such as dry cough, prolonged sputum production, difficulty breathing, persistent coughing up blood or repeated lung infections.
5.2 Treatment of chronic obstructive pulmonary disease (COPD) To treat COPD, there are 2 methods: medication and non-drug therapy:
Non-drug treatment: Includes physical therapy and oxygen therapy Drug therapy : Two main groups of drugs will be applied: Bronchodilators: Parasympathetic nervous system depressants, beta 2 receptor stimulants and Xanthin group. Corticosteroids: There are injections, oral and inhaled. During acute episodes, additional antibiotics may be required to fight infection. Chronic Obstructive Pulmonary Disease (COPD) is chronic (not completely cured) and often has acute exacerbations due to infection or viral infection. Although the disease cannot be completely cured, it can be partially controlled as well as slow its progression over time. The goal of treatment is how the patient can best live with the disease. If the treatment goes well, the patient can lead a near-normal life (still taking medication) but rarely have exacerbations requiring hospitalization.

Người bệnh nên đến cơ sở y tế uy tín để được thăm khám và điều trị
To register for examination and treatment at Vinmec International General Hospital, you can contact Vinmec Health System nationwide, or register online HERE
Recommended video:
Health check recurring at Vinmec: Protect yourself before it's too late!
SEE MORE
What is the difference between lymph node tuberculosis and pulmonary tuberculosis? How many types of tuberculosis are there? What disease does a persistent dry cough warn of?