This is an automatically translated article.
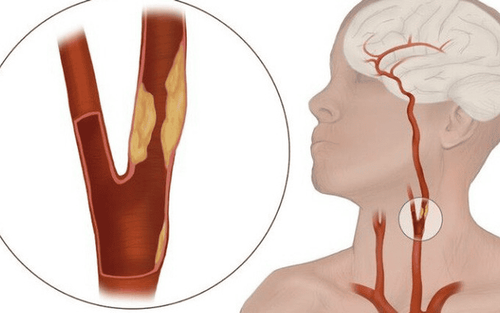
Nodular arteritis affects each segment of blood vessel, mainly in small and medium arteries. If not detected and treated promptly, the disease can cause complications of kidney failure, heart attack, stroke,...1. What is nodular arteritis?
Polyarteritis nodosa, also known as polyarteritis nodosa or PAN, is inflammation and necrosis of small blood vessels, typically small and medium sized arteries. The disease causes symptoms depending on the location of the damaged blood vessel. Lesions can affect almost any organ, but are most common in the skin, liver, kidneys, heart, gastrointestinal tract, nerves (central and peripheral nervous system), muscles, and testes.Nodular arteritis is a rare disease that can occur at any age, the rate is higher in people 50 - 60 years old, the male/female ratio is 2.5/1.
2. Causes of nodular arteritis
Currently, the cause of arteriosclerosis is still unknown. However, studies have shown a number of factors that increase the risk of disease such as:CECR1 gene mutations; HBV infection (present in 30% of cases), HCV, Varicella-zoster virus, parvovirus B-19,...; Infections: Tuberculosis, Klebsiella, Pseudomonas, Toxoplasma gondii,...; Taking drugs: Minocycline, Levamisole, Thiabendazole, hepatitis B vaccine,...
3. Symptoms of polyarteritis nodosa

Sốt có thẻ là triệu chứng của viêm đa động mạch nút
3.1 Systemic symptoms Fever; Pale, tired people; Anorexia, weight loss. 3.2 Skin symptoms Skin symptoms are quite common, occurring in about 40% of patients with arteritis nodule. Characteristic manifestations include:
Nodules, mainly in the lower extremities, with lesions similar to erythema nodosum but smaller lumps; Ulcers: Usually occur on lumps, when healed without leaving skin atrophy; Liveoid network: These are blue-violet reticular patches on the skin, often distributed around the fat lobes, which are more obvious when experiencing cold, bleeding; If you have acute arteritis, you may have symptoms such as large inflammatory plaques, edema; Raynaud's syndrome, ischemia of the extremities, especially in the toes, causing gangrene; Skin lesions are often painful, mainly in the lower extremities. 3.3 Symptoms on other organs Joint pain, muscle pain, especially leg muscles; Central nervous system: Infarction, cerebral hemorrhage. May present late (2-3 years after vasculitis); Peripheral Nerves: Asymmetrical peripheral neuritis; Gastrointestinal: Atypical symptoms include abdominal pain, vomiting, gastrointestinal bleeding, hepatitis, cholecystitis, mesenteric infarction, intestinal perforation, pancreatitis,...; Kidney: Decreased kidney function, increased blood pressure; Testicular - ovary damage: Unilateral epididymitis; Cardiovascular: Chest pain, pericarditis, myocarditis, arrhythmia, myocardial infarction; Other manifestations: Blurred vision, signs of infarction / rupture of aneurysms in other organs.
4. Treatment of polyarteritis (PAN)
4.1 Using corticosteroids: High doses of prednisone or solumedrol as prescribed by your doctor. After 1 month, the dose of prednisone may be reduced if the patient's condition and erythrocyte sedimentation rate improve. Gradually reduce the dose of prednisone over the next 12 months until it is completely stopped. Where prednisone is required in combination with cyclophosphamide, the corticosteroid dose should, if possible, be reduced more rapidly to reduce the risk of infection. The patient's hematology and renal function should be checked frequently when cyclophosphamide is administered orally or intravenously. Dosage should be adjusted according to each case. Note: The potential toxicity of cyclophosphamide may increase the risk of bladder cancer, hematologic malignancies, hemorrhagic cystitis, bladder fibrosis, hypogonadism, bone marrow suppression. Cyclophosphamide is generally not recommended in patients with hepatitis B-associated nodal arteritis because the combination of steroids with cyclophosphamide may increase viral replication; Tumor necrosis factor inhibitors: Monoclonal antibodies such as adalimumab (Humira), certolizumab pegol (Cimzia), infliximab (Remicade) and golimumab (Simponi); Adjuvant therapy: In cases of intravenous cyclophosphamide use, concomitant mercaptoethane sulfonate (MESNA) should be used; Inpatients require stabilization of the initial condition, and treatment depends on the extent of disease and organ damage.
Điều trị viêm đa động mạch bằng thuốc
4.3 Long-term care for the patient Monitor blood counts, urinalysis, renal and liver function tests; Closely monitor infectious complications; Early detection of slow-onset cancers, especially in patients treated with cyclophosphamide; Maintain a low-salt diet if the patient has hypertension.
5. The danger of nodal arteritis
The disease may be localized to a single organ or progress to multiple organ failure. Complications of polyarteritis nodosa include renal failure, thrombosis of the involved vessels, tissue and organ necrosis, myocardial infarction, stroke, multifocal mononeuritis, and peripheral neuropathy. border, perforation of hollow viscera (intestine).
If left untreated, nodular arteritis has a poor prognosis. It is estimated that the 5-year survival rate of patients is only about 13%. If treated with steroids and cytotoxic drugs, the 5-year survival rate can be as high as 75-80%. Patient survival was improved with hepatitis B-associated polynoditis due to the introduction of antiretroviral regimens. Prognosis is poorer in patients with polyarteritis with proteinuria, renal failure, gastrointestinal tract lesions, central nervous system involvement, or cardiomyopathy.
Nodular arteritis is a dangerous disease with many unpredictable complications and a rather poor prognosis. Therefore, as soon as the warning symptoms appear, the patient should go to the hospital for examination, accurate diagnosis and timely and effective treatment plan.
Vinmec International General Hospital is one of the hospitals that not only ensures professional quality with a team of leading medical doctors, modern equipment and technology, but also stands out for its examination and consultation services. comprehensive and professional medical consultation and treatment; civilized, polite, safe and sterile medical examination and treatment space.
To protect cardiovascular health in general and detect early signs of cardiovascular disease, customers can sign up for the Cardiovascular Screening Package of Vinmec International General Hospital. The examination package helps to detect cardiovascular problems at the earliest through tests and modern imaging methods. The package is for all ages, genders and is especially essential for people with risk factors for cardiovascular disease.
Why should you choose Cardiovascular Screening Package at Vinmec International General Hospital?
Simple and quick procedure. Enthusiastic advice and support, reasonable and convenient examination process. Comprehensive facilities, including a system of clinics and consultations, blood collection room, dining room, waiting area for customers... The medical staff has high professional qualifications, style. Professional, caring way of working.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.