This is an automatically translated article.
The article was professionally consulted by Doctor Nguyen Ngoc Bach - Respiratory Internal Medicine Doctor, Vinmec Times City International General Hospital.Asthma is a chronic respiratory disease with a high incidence, especially in children. There are many methods applied in the diagnosis of bronchial asthma today, including the technique of measuring NO concentration.
1. NO gas biology
Nitric oxide (NO) has been known as a gas found in environments polluted by vehicle exhaust and cigarette smoke. Recently, the role of NO in exhaled breath has been known as an inflammatory marker, which helps to reflect many different pathological conditions of the respiratory system, especially asthma.NO gas is generated from the reaction of converting L-arginine to L-citrulline with the catalysis of the enzyme NOS (nitric oxide synthase). There are three types of NOS enzymes: eNOS (endothelial NOS), iNOS (inducible NOS) and nNOS (neuronal NOS).
In asthmatic patients with atopy, there is an increase in the synthesis of iNOS in bronchial epithelial cells, thereby increasing the concentration of NO in the bronchial wall. NO from the bronchial wall diffuses into the bronchial lumen due to the concentration difference. Therefore, fraction of exhaled nitric oxide (FeNO) is considered as a direct biomarker for the TH2-type inflammatory response (or eosinophilic inflammation) in patients with bronchial asthma.

NO trong khí thở là một chất chỉ điểm tốt cho quá trình viêm của đường hô hấp, nhất là trong chẩn đoán hen phế quản.
2. The role of measuring NO gas concentration in the diagnosis of bronchial asthma, bronchial hyperreactive syndrome?
The detection of nitric oxide (NO) in exhaled air and measurement of NO concentration in exhaled air play an increasingly important role in the diagnostic and therapeutic strategies of Asthma. An increase in NO concentration in exhaled air directly reflects inflammation either in the bronchi or in the alveoli. Furthermore, NO in inhaled air is an early marker of airway inflammation.Therefore, the measurement of exhaled NO helps to diagnose bronchial asthma in the latent stage. Elevated exhaled NO concentrations seem to occur earlier than respiratory dysfunction as determined by pulmonary function tests.
Furthermore, measurement of exhaled NO is more specific and sensitive than eosinophil count or soluble interleukin (IL) concentration in diagnosing the severity of bronchitis. management on patients. In addition, a correlation between increased NO concentration in breathing air and severity of bronchial hyperresponsiveness syndrome has been demonstrated.
Compared with other tests that evaluate inflammation (e.g. eosinophils in sputum, bronchoalveolar lavage or biopsies), NO measurement has many advantages because it is easy to perform, does not invasive and precise. In addition, because of its ease of implementation, the measurement of NO in exhaled breath is a useful tool in screening and detecting asthma patients in the community. The arrival of compact new generation meters also allows this measurement to be performed in the clinic, emergency department or in the patient's home.
Measurement of exhaled NO (FeNO: fraction of exhaled nitric oxide) is a simple, rapid, non-invasive and highly reliable test. FeNO is expressed in units of ppb (parts per billion), which is equivalent to one billionth of a liter of NO per liter of exhaled air. FeNO reflects certain inflammatory mechanisms (among many) of asthma that respiratory function cannot. Therefore, FeNO serves the needs of individualizing asthma treatment: detecting groups of patients with inflammatory mechanisms capable of responding to inhaled corticosteroids (ICS: inhaled corticosteroids) or other specific anti-inflammatory drugs; Avoid ICS in patients who are unlikely to respond.
3. How is NO concentration measured?
FeNO measurement is the measurement of NO concentration from the lower respiratory tract. The nasal region has a relatively higher concentration of NO than the lower respiratory tract. Therefore, techniques for measuring NO in the lower airways should avoid sampling NO-containing gases from the nasal region. Normally, FeNO fluctuates widely among people but is stable for each person. Factors that can affect FeNO: age (in children: FeNO increases with increasing age); gender (male is taller than female); height (increasing as height increases); smoking status (reduced by smoking); medications you are taking (especially ICS, montelukast, L-arginin); and expiratory flow (decreases as flow increases).FeNO is elevated in asthmatic patients compared with normal people. Repeated measurement of FeNO during the steady-state phase in asthmatics can determine the normal FeNO value of each patient. FeNO is also elevated in people with atopy, whether asthma or not. In patients with chronic obstructive pulmonary disease (COPD), FeNO is decreased during the steady-state period when treated with ICS and elevated during the exacerbation. FeNO may be elevated in the following conditions: bronchiectasis, viral respiratory infections, systemic lupus erythematosus, cirrhosis, organ rejection disease. FeNO is decreased in the following diseases: HIV infection, pulmonary hypertension, cystic fibrosis.
FeNO tăng cao ở bệnh nhân hen phế quản so với người bình thường
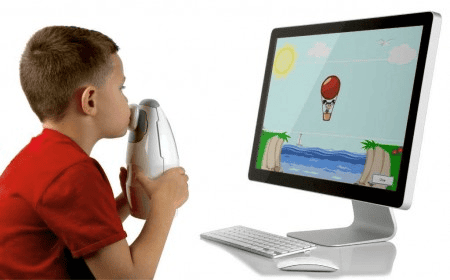
Direct measurement is that the patient breathes directly into the NO meter. Measured results including: expiratory volume, expiratory flow, expiratory time, expiratory pressure ... are recorded and analyzed on the machine right at that time. We can take measurements at 1 expiratory flow rate or with different expiratory flow rates. With multiple expiratory flows allowing the assessment of NO concentration in the alveoli, the ability of NO to diffuse across the bronchial wall thus allows a direct assessment of the anatomical origin of exhaled NO. However, this measurement method requires the presence of the patient next to the meter, as well as equipment for each respiratory function, so this measurement method is only performed in a few large hospitals. and some labs. The "indirect" way of measuring NO is to measure the distance in space and time, which allows to overcome the disadvantages of the direct measurement method. The patient's breathing air is collected into an air bag made of Mylar material - a material that does not react with any gases present in the breathing air. The NO concentration in the bag was then measured within 12 h from the time the patient breathed into the bag.
4. The value of NO in the diagnosis and treatment of bronchial asthma
FeNO is recommended as a biomarker to diagnose asthma, monitor response to inhaled corticosteroids (ICS), adjust ICS dose, verify adherence, and predict impending exacerbations. When FeNO is combined with spirometry, the sensitivity and specificity in the diagnosis of asthma can be as high as 94% and 93%. FeNO is more predictive of response to corticosteroids than spirometry, bronchodilator testing, peak flow variability, or methacholine bronchostimulation testing.Low FeNO is a reliable indication that a TH2-type inflammatory response is absent. Excluding the presence of airway inflammation is helpful in interpreting the patient's symptoms. For example, in patients with uncontrolled asthma, low FeNO helps physicians focus on finding other diagnoses (such as obesity, GERD, or an anxiety disorder) rather than increasing the dose of ICS unnecessarily. FeNO responds rapidly and corresponds to the daily dose of ICS. That means FeNO tells us what to expect when we start or increase the dose of ICS.
In summary, measurement of NO is an effective measurement that allows non-invasive exploration of the inflammatory process of the airways, and is now becoming an important tool in the diagnostic and therapeutic strategy of asthma. bronchi.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.