This is an automatically translated article.
Posted by Doctor Vo Ha Bang Suong - Therapist - Department of Examination & Internal Medicine - Vinmec Phu Quoc International General Hospital
Melioidosis, also known as Whitmore's disease, or "Vietnam time bomb". The disease is caused by the bacterium Burkholderia pseudomallei. The bacteria are found in soil and water in tropical regions, especially in Southeast Asia and northern Australia. Humans and other animals become infected by exposure to this bacteria in the environment.
1. Characteristic signs of Whitmore .'s disease
Melioidosis is characterized by fever, pneumonia, and abscesses, ranging from mild, localized infections to sepsis and rapid death.
The diagnosis of melioidosis is challenging because it resembles many other diseases, especially tuberculosis. Accordingly, the diagnosis of the disease requires high suspicion from the clinical presentation and must be confirmed by culture.
Aggressive intravenous antibiotic therapy is the mainstay of therapy in most patients and may be required for several weeks, depending on the clinical picture. Followed by oral radical therapy for a minimum of 3 months.

Bệnh Whitmore gây ra các triệu chứng viêm phổi
2. Epidemiology of Whitmore .'s disease
Cause of disease : The disease is caused by bacteria Burkholderia pseudomallei. B. pseudomallei is a gram-negative bacillus. Exists in soil, water, air (dust) environments under different environmental conditions. The body is more susceptible to disease in extreme climatic and weather conditions: Rain, storms. Infectious source: The infectious source of the disease exists in nature. Bacteria are present in soil, polluted water, and dust in the air. Transmission route: Most are thought that the disease is transmitted mainly through skin, mucous membranes when in contact with bacteria present in soil, water, and dirt when exposed without protective means (farmers do working in the fields, people who come into contact with dirty soil and water like soldiers...). SEE ALSO: Risk of spread of Whitmore's disease
Other transmission routes are mentioned: Through inhalation when breathing dust containing bacteria, through ingestion when drinking contaminated water sources. It is possible that the patient presents with an unidentified, latent infection. In practice, it is often difficult to determine exactly when, where, and how infection occurs, especially when people are constantly exposed to bacteria and the environment. Direct person-to-person, human-to-animal transmission rarely occurs.
Geographical distribution: Melioidosis is a disease of Southeast Asia and northern Australia, but over the past 20 years, the disease has increasingly appeared in tropical regions, including the Indian subcontinent, the Asian region Sub-Saharan Africa, Central and South Africa and the Caribbean. The largest number of cases were recorded from Thailand (especially in the northeast), Malaysia, Singapore and northern Australia. Increasingly, the disease is being recognized in different countries around the globe. Season: the disease is highly seasonal, peaking in the rainy season corresponding to the time of most exposure. Age, sex: The disease occurs in all age groups, the most common is the adult age (from 40-70 years old). The disease is more common in men than in women, less often in young children, many children have localized infection, which is relatively mild. Risk factors: In the adult population, approximately 55 to 80% of patients have underlying medical conditions that make them susceptible to melioidosis, especially diabetes; chronic kidney, liver or lung disease; drinking too much alcohol or binge eating; corticosteroid use; or hemolytic anemia, the patient is being treated for cancer.
3. Pathogenesis
Clinical manifestations reflect the wide range of clinical manifestations that infection can cause, depending on the balance between the size and route of initial infection as well as the effectiveness of the host response. Initially, bacteria multiply at the entry site, which can lead to local lesions such as skin pain with connective tissue inflammation, abscess formation, or pneumonia.
This condition clears up in some patients, but in many others the bacteria can spread through the bloodstream or lymphatic system, resulting in secondary damage almost all over the body, but especially the in the lymph nodes, liver, spleen, lung and prostate gland (in men)
The course of the disease can be very variable, with some patients developing acute and fulminant infections and others developing The development of chronic, painless, granular lesions may sometimes be asymptomatic.
MORE: Whitmore's disease: Who is at risk?
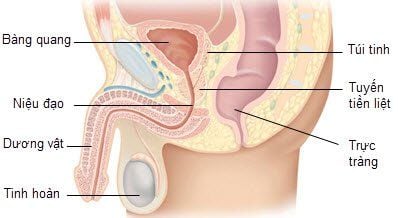
Tuyến tiền liệt ở nam giới có thể bị tổn thương do bệnh whitmore gây ra
4. Clinical forms
Acute melioidosis (85%): incubation period from 1 to 21 days (median 9 days) Chronic melioidosis (11%): defined as symptomatic disease with a duration of presentation longer than 2 Months Disease progression from a previous asymptomatic latent infection (4%) Acute form
Manifestations of systemic infection
Fever: >39 degrees Celsius Infectious facial expression, fatigue. Severe manifestations of septic shock: The pulse is fast, small, difficult to detect or very slow. Blood pressure drops, clamped, not measured. Spot expressions
4.1. Pneumonia
Pneumonia is the disease with the highest rate. Patients with sepsis often have fever, fatigue, cough, and chest pain. Clinical examination showed the following:
Chest radiograph: There was diffuse nodular infiltrates that could be in both lung fields, lesions progressed rapidly. Or there is consolidation of 1 or 2 lobes of the lung. Subacute or chronic pneumonia: Tuberculosis-like presentation with fever, weight loss, cough with sputum, sometimes hemoptysis, upper lobe infiltrates with or without cavitation on radiographs.
4.2. Urinary tract infection
Manifestations of pain in the renal fossa, painful urination
Urinalysis: white blood cells, red blood cells, proteinuria Ultrasound of abdomen, pelvis, prostate: inflammatory lesions. Determined by CT scan of the abdomen with contrast.
4.3. Skin damage
There are often ulcers, widespread necrosis (so people call it a flesh-eating bacteria disease)

Bệnh Whitmore thường gây ra hiện tượng lở loét
4.4. Infectious arthritis and osteomyelitis
Symptoms and signs of arthritis and osteomyelitis may be the initial presentation that causes a patient to be hospitalized for treatment. Accordingly, the knee joint is the most common site of infection, followed by the ankle, hip joint and shoulder joint
4.5. Inflammation of the brain, spinal cord, meninges
Encephalitis, meningitis will be less common. Manifestations are similar to those of meningitis caused by other infections.
It is often difficult to culture and identify B. Pseudomalei in CSF. Indicators such as increased white blood cells, dominant Lymphocytes were recorded. Therefore, it is essential to identify B.Pseudomalei in any implicated body secretions implicated. It is very important for treatment attitude and relapse prevention.
4.6. Inflammation of the lymph nodes
Inflammation of the lymph nodes manifests as hot, red, swollen, pus-filled swelling that can be easily seen in the lymph nodes of the neck, armpit, and groin. However, some inconspicuous locations can be difficult to spot.
4.7. Abscesses
Abscesses at locations: Liver, spleen, kidney, muscle...
4.8. Parotid salivary gland inflammation
Parotid salivary gland inflammation occurs mainly in children. The clinical picture of acute parotid gland inflammation, with fever, increased white blood cell count in blood tests. Some studies have recorded a prevalence of about 43% in children in Thailand and Cambodia.
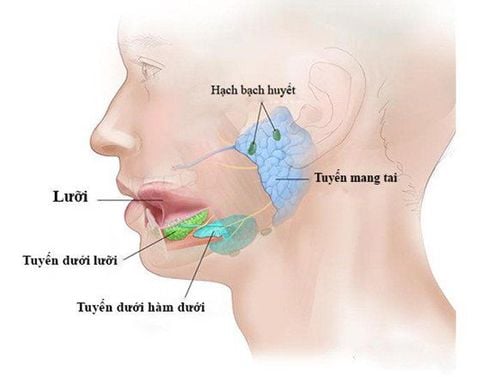
Viêm tuyến nước bọt mang tai là một thể bệnh của bệnh Whitmore
5. Diagnosis of Whitmore .'s Disease
5.1. Diagnosis of the disease based on bacterial culture is the gold standard
Using Ashdown's agar containing gentamicin allows selective growth of B.pseudomallei . Specimens include: blood, sputum, throat swabs, rectal swabs, skin lesions and sores, abscesses. Indirect hemagglutination test, ELISA does not have much meaning. People living in endemic areas may have high background antibodies. A negative result is also not significant in excluding disease. PCR: specificity and positive predictive value are both high, but negative tests cannot rule out the possibility of infection. In addition, there are other supporting tests such as: Blood cell analysis, Stool analysis. Urine cytology X-ray, CT scan of the lungs, Ultrasound of the abdomen, CT scan of the abdomen, CSF
5.2. Differential diagnosis
Whitmore's disease is easy to confuse with other diseases, so it is necessary to think of B.Pseudomalei in the diagnosis. Some diseases need to be differentiated such as: Community-acquired pneumonia, tuberculosis. Sepsis caused by other bacteria. Diseases caused by leptospira, Ricketsia, malaria.
6. Treatment of Whitmore's Disease
Mortality in melioidosis without specific antibiotic therapy can be >50% and >90% if the patient is in septic shock. Even with appropriate antibiotics, delays in diagnosis and critical care treatment lead to a mortality rate of about 40% in many endemic areas.
Once the diagnosis is confirmed, antibiotic therapy is divided into 2 phases: aggressive intravenous antibiotic attack, followed by oral eradication phase.

Bệnh nhân mắc bệnh Whitmore đều cần sử dụng thuốc kháng sinh
6.1. Active antibiotic therapy (attack phase)
Intravenous antibiotic therapy with ceftazidime, meropenem or imipenem/cilastatin should be instituted. In patients with purulent (including skin and visceral abscesses/ulcers) and in bone/joint, urogenital (but not pneumonia) infections, trimethoprim/supplementation may be recommended. sulfamethoxazole orally or intravenously (if available).
Combination use of folic acid should be considered when high-dose trimethoprim/sulfamethoxazole is given for a long time to reduce the potential for adverse events related to the drug's anti-folate action (eg, bone marrow toxicity).
Duration of treatment is determined by severity and clinical features. Duration is at least 10 to 14 days and should be extended to 4 weeks if:
Pneumonia requiring admission to the intensive care unit, or pneumonia associated with mediastinal lymphadenopathy or chest X-ray lesion spread on both sides. Visceral abscess, septic arthritis, or other deep visceral pus-filled conditions, with a 4 week period from the last aspiration (eg, with a prostate abscess or inflammatory bowel disease). infected joints). This interval should be extended to 6 weeks (minimum) if osteomyelitis is present. In addition, this interval should be extended to 8 weeks if the patient has neurogenic melioidosis or fungal aneurysms.
If because of the condition does not prolong the treatment, then the therapy should be at least 10-14 days. In this case, it is important to complete the complete oral curative regimen.
Select drugs and dosage as follows:
Ceftazidime: children: 50 mg/kg IV every 6-8 hours, maximum 8 g/day; Adults: 2 g IV every 6-8 hours. Or:
Meropenem: children: 25 mg/kg IV every 8 hours, up to 3 g/day; Adults: 1 g IV every 8 hours Double dose in patients with neurogenic Melioidose Or:
Imipenem/cilastatin: children: 25 mg/kg IV every 6 hours, up to a maximum of 4 g/day; Adults: 1 g IV every 6 hours
6.2. Radical therapy
Oral trimethoprim/sulfamethoxazole is the treatment of choice. Combination use of folic acid should be considered when high-dose trimethoprim/sulfamethoxazole is given over a long period of time to reduce the possibility of adverse events related to the drug's anti-folate action (eg, bone marrow toxicity). However, bone marrow suppression, rash, and increased serum potassium and creatinine are common in patients with melioidosis treated with trimethoprim/sulfamethoxazole. Alternative radical therapy for these patients is amoxicillin/clavulanic acid, or doxycycline (adults only).
In children over 2 months of age and pregnant women, trimethoprim/sulfamethoxazole is still the drug of choice, although you may consider deferring trimethoprim/sulfamethoxazole until beyond the first trimester due to concerns about its teratogenic potential. Amoxicillin/clavulanic acid is an alternative, although it is associated with a relatively high risk of recurrence.
Patients should continue on curative therapy for a minimum of 3 months and up to 6 months if neurogenic melioidosis or osteomyelitis is present. Some patients with localized disease (defined by ultrasonography to rule out other foci) and generally feeling well can be safely treated with either oral curative therapy.
Selection and dosage are as follows:
Priority 1: Trimethoprim/sulfamethoxazole: children: 6-8 mg/kg orally twice a day; adults weighing <40 kg: 160 mg orally twice a day; adults weighing 40-60 kg: 240 mg orally twice a day; adults weighing >60 kg: 320 mg orally twice a day
Dosage relates only to the trimethoprim component. This indication requires a higher than normal dose.
Option 2:
Amoxicillin/clavulanate: children: 20 mg/kg orally three times a day; adults weighing <60 kg: 1000 mg orally three times a day; adults weighing >60 kg: 1500 mg orally three times a day Dosage is based on amoxicillin composition only. The required amoxicillin to clavulanate ratio of 4:1 is required for this indication, i.e. a higher than normal dose is required Doxycycline: adult: 100 mg orally twice daily

Thuốc Trimethoprim được sử dụng trong liệu pháp tiệt căn nhằm điều trị bệnh Whitmore
6.3. Combination therapy on diseases
Treat abscesses
Accumulation sites should be drained if possible (especially prostate and muscle abscesses and large liver abscesses), but splenic abscesses usually do not require drainage. Ideally, intravenous therapy should be timed from the last drainage of positive cultured pus.
Septic shock from melioidosis
Resuscitation and intensive care therapy should be instituted according to guidelines for severe sepsis.
7. How is Whitmore's disease prevented?
Currently, there is no vaccine for Whitmore's disease. Accordingly, the current most effective prevention methods to protect and prevent to reduce the risk of disease transmission are as follows:
Avoid direct contact with soil or foreign environment People working in contact with contaminated soil and water in the environment must wear protective equipment including rubber gloves, boots or wading boots, wash hands with soap and clean water immediately after exposure In case of injury contaminated with soil or in the environment, immediately wash the wound with soap and water Cover open wound and avoid contact with soil or water until completely healed. Do not apply herbs or other substances to the wound. In case the wound comes into contact with soil or the environment, wash the wound thoroughly with soap and water. Always wear shoes. Do not go barefoot Drink only bottled or boiled water. Do not drink untreated water. Food hygiene. Avoid contaminated food. Food must be cooked. When outdoors, avoid heavy rain or dust clouds. If caught in a cloud of dust, cover your mouth and nose. Use an umbrella to protect yourself from the rain. Don't smoke, quit drinking. Increases body's resistance The risk of melioidosis is higher if you have certain conditions, including diabetes, chronic kidney disease, and conditions that require treatment with corticosteroids or drugs that suppress the immune system. These objects are advised to avoid being outdoors during periods of heavy rain and strong winds.
With many years of experience in the examination and treatment of diseases, now at Vinmec International General Hospital, it has become one of the major health care centers, capable of examining, screening and treatment of many specialized diseases. Therefore, if you have signs of Whitmore's disease, you can go to Vinmec International General Hospital to examine and receive support and advice from doctors.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.