This is an automatically translated article.
The article is professionally consulted by Master, Doctor Phan Ngoc Toan - Emergency Medicine Doctor - Emergency Department - Vinmec Danang International Hospital.Severe hypoxia and cardiovascular collapse, leading to cardiac arrest, cerebral ischemia, and death are the most common complications associated with intubation.
1. What is difficult intubation?
As defined by the American Society of Anesthesiologists (ASA), difficult intubation is a duration of intubation that takes more than 10 minutes or requires more than three attempts2. Expected difficult intubation
Factors predicting difficult intubation are related to examination of the head, face, neck, and oral cavity. This is a very important examination, it helps the emergency physician to predict whether intubation is difficult or easy...2.1 Mallampati's grading scale This assessment is done when the patient is in the sitting position. , neck back, mouth open, tongue sticking out and beginning to pronounce "A". There are 4 degrees as follows:
I: Visible hard palate, soft palate, uvula, posterior pharyngeal wall, anterior and posterior column Amygdales. II: Hard palate, soft palate, part of the uvula and posterior wall of the pharynx are seen. III: Hard palate, soft palate and base of the uvula are seen. IV: Only hard palate is visible. If grade III and IV is difficult intubation.

Hình 1 – Phân độ Mallampati
Grade 1: When the entire gap between the two vocal cords is visible. Grade 2: When only the posterior part of the larynx is visible. Grade 3: When only epiglottis cartilage is visible. Grade 4: When only the soft palate is visible. At grade 3, 4, it can be concluded that intubation is difficult.
2.3 Chin - thyroid distance This distance is defined from the superior edge of the thyroid cartilage to the mid-chin. Measure in sitting position, neck straight, inhale. If this distance is < 6cm (3 fingers) it is difficult to intubate.
2.4 Distance between 2 dental arches The distance between 2 teeth is measured at the maximal opening position, if < 3cm, it is difficult to intubate.
2.5 Other signs There are also some other signs to recognize difficult intubation such as:
Short neck. Lower jaw small, tapered back. High palate, upper front teeth protruding (protruding teeth). Narrow oral cavity, large tongue (in children). Breasts, breasts are too big, obese. Limited movement of the temporomandibular joints, cervical spine. Tumors on the palate, pharynx, larynx.

Hình 2 – Phân độ Cormack và Lehance
3. Difficult intubation techniques
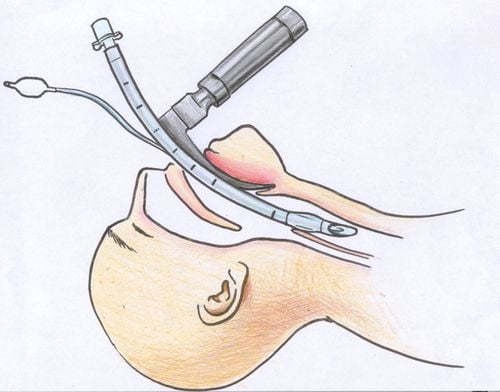
3.1 Change the patient's position Elevate the patient's head with a small pillow so that the axis of the oral cavity and the larynx form a straight line. An assistant presses the laryngeal cartilage posteriorly and upward. The other person helps pull the upper lip back to see the larynx more clearly. 3.2 Use an endotracheal tube or guide rod Use an endotracheal tube (Mandrin or Stylet) inserted into the endotracheal tube to bend the endotracheal tube in a cane or S shape for easier insertion.
Use a guide with a soft end, put it in the trachea first, then insert the endotracheal tube along this stick.
3.3 Intubation through the nose Insert the endotracheal tube about 10cm through the nose and then gently push it in, the patient inhales while checking the patient's exhaled breath through the endotracheal hole in the expiratory phase out.
When the endotracheal tube passes through the vocal cords, the patient will have a cough reflex and some air will come out of the tube. Check the position of the placed tube by squeezing the balloon and listening to the lungs, then immobilize the tube.
3.4 Other methods In addition, there are a number of methods applicable to difficult intubation such as:
Retrograde intubation. Use a flexible bronchoscope for endotracheal intubation. Use a laryngeal mask. Open the pericardial membrane for ventilation. Open the trachea.

Hình 3 – Trình tự đặt nội khí quản chuỗi nhanh
Difficult intubation situations require the anesthesiologist to anticipate the problem, plan the initial management, and identify alternate floors to be used if unforeseen difficulties are encountered. At any point in the procedure, the anesthesiologist should always choose the technique with which he or she is most comfortable and has the most experience.
Any questions that need to be answered by a specialist doctor as well as if you have a need for examination and treatment at Vinmec International General Hospital, please book an appointment on the website to be served.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.