This is an automatically translated article.
Posted by Master, Doctor Mai Vien Phuong - Gastrointestinal Endoscopy - Department of Medical Examination & Internal Medicine - Vinmec Central Park International HospitalAbbreviations:
Upper Gastrointestinal Bleeding (UGIB)
Varicose Vein Upper Gastrointestinal Bleeding (NVUGIB)
Varicose Upper Gastrointestinal Bleeding (VUGIB)
Upper Gastrointestinal Bleeding is defined as bleeding originating from the esophagus to the ligament of Treitz of the duodenum and is classified as gastrointestinal bleeding not due to ruptured varices and bleeding due to ruptured varices.
1. Frequency of upper gastrointestinal bleeding and current means of hemostasis
Upper gastrointestinal bleeding from varicose veins remains a common clinical problem globally. It is associated with high mortality, morbidity and costs of the health care system. Despite the continued improvement of therapeutic endoscopy, the 30-day rate of recurrent bleeding and associated mortality is an ongoing problem. The Food and Drug Administration currently has approved conventional or conventional therapeutic endoscopic modalities including epinephrine injection, argon coagulation, heating probes, and OTSC bronchoscope clamps, which can used alone or in combination to reduce the risk of bleeding.2. New endoscopic means of hemostasis
Recently, new advanced endoscopic devices have received more attention for initial treatment of bleeding lesions and as an adjunct when conventional therapies fail to achieve hemostasis. This review highlights emerging endoscopic modalities used in the management of upper gastrointestinal bleeding due to varicose veins such as over-the-scope clips (OTSCs), Coagrasper, hemostatic sprays, and excision. Radiofrequency ablation, cryotherapy, endoscopic flexible gastrointestinal suture devices and endoscopic ultrasound therapy for arterial occlusion.
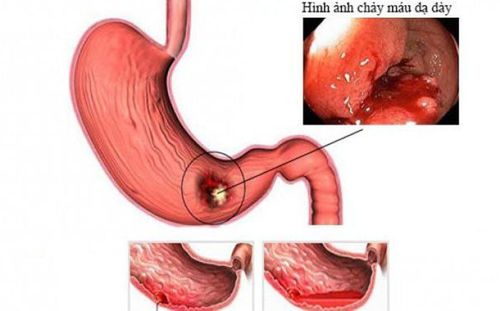
Chảy máu đường tiêu hóa sẽ rất nguy hiểm nếu không can thiệp sớm
3. Causes of upper gastrointestinal bleeding not due to ruptured varicose veins
Gastrointestinal bleeding is a medical emergency that leads to significant morbidity, mortality, and healthcare costs. It may present as a life-threatening major hemorrhage or chronic silent bleeding. Upper gastrointestinal bleeding (UGIB) is defined as any gastrointestinal bleeding that originates above the ligament of Treitz. UGIB can be further classified as varicocele upper gastrointestinal bleeding (NVUGIB) and varicocele upper gastrointestinal bleeding (VUGIB). Common causes of varicocele-related upper gastrointestinal bleeding are listed in Table 1. The morbidity and mortality associated with varicose veins-related upper gastrointestinal bleeding have decreased as a result of advances. in the prevention and management of upper gastrointestinal bleeding due to varicose veins. However, it remains a common clinical problem with an annual incidence of about 90-108 per 100000 and a mortality rate of 3% to 14%.Table 1 Etiology of upper gastrointestinal bleeding due to ruptured varicose veins.
| Loét / viêm | Bệnh viêm loét dạ dày |
| Ăn mòn thực quản, viêm dạ dày hoặc viêm tá tràng | |
| Loét miệng nối (sau phẫu thuật cắt dạ dày) | |
| Tổn thương mạch máu | Dị sản mạch máu hang vị ( Gastric antral vascular ectasia) |
| Tổn thương của Dieulafoy | |
| Dị dạng mạch / Dị dạng động mạch | |
| Rò động mạch chủ-ruột | |
| Bệnh dạ dày sung huyết | Bệnh dạ dày tăng áp cửa |
| Tổn thương ác tính | Khối u mô đệm đường tiêu hóa (GIST) |
| Không phải GIST ( ví dụ: Lipoma, schwannoma) | |
| Ung thư dạ dày và thực quản | |
| Tổn thương di căn ở đường tiêu hóa trên | |
| Chảy máu sau thủ thuật | Nội soi cắt niêm mạc và bóc tách dưới niêm mạc |
| Sau phẫu thuật cắt cơ vòng của ERCP | |
| Khác | Hội chứng Mallory Weis |
| Loét Cameron |
4. The role of early interventional endoscopy
Early endoscopic intervention within 24 h of presentation significantly improved patient outcomes and was not significantly different from those who received endoscopic intervention < 12 h after symptom onset. When endoscopy is performed, it is important to have a standard method for diagnosing the cause of bleeding, assessing for signs of recent bleeding (i.e. active bleeding, visible blood vessels). presence of blood clots, red or black spots covering the ulcerative lesion) and gastric ulcer classification according to the Forrest classification. Endoscopy is important in revealing the etiology of varicose veins in the upper gastrointestinal tract.4.1. Traditional method - epinephrine hemostasis The development and widespread use of endoscopy has contributed mainly to reducing the need for surgery and the morbidity associated with varicose veins in the upper gastrointestinal tract. Endoscopic management is classified as injectable, thermal, and mechanical. Among the traditional methods, epinephrine injection is the most common and widely used modality because of its feasibility to perform and the need for less coordination between the endoscopist and assistant. However, epinephrine alone is less effective than in combination with heat or mechanical and other monotherapy such as forceps, transducers, and electrodynamics.
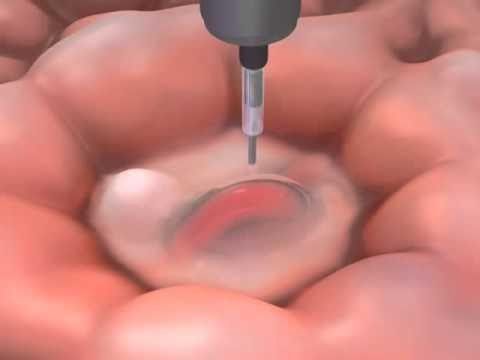
Kỹ thuật tiêm cầm máu qua nội soi
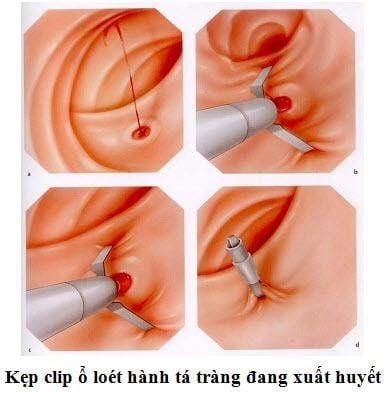
Furthermore, tissue damage is minimal with clips and ulcer healing is unhindered. Introduced in clinical practice in the 1990s, over the years, the endoclip has evolved in functionality (such as accuracy, tensile strength, rotation, overshoot, and closure strength). ), physical characteristics and cost. The recently published study by Wang et al compared the function of five different types of hemostatic forceps. According to the research results, Resolution 360 (Boston Scientific, Marlborough, Mass) was the fastest clip recorded by surgeons. Instinct (Cook Medical, Bloomington, Ind.) was found to be mechanically stronger and works better at compressing thick, fibrous tissues and scarred ulcers. Rotation and jerking (defined as >30° and >1 half a turn, respectively) tend to occur when clips are rotated in the same direction. As for the clip firing rate, the 16mm SureClip performs well when compared to other through-pipe clamps.
Chảy máu tái phát sau can thiệp
Table 2: Summary of new endoscopic modalities for the management of varices-associated upper gastrointestinal bleeding.
| Tiêm cầm máu | Nội soi siêu âm hướng dẫn liệu pháp điều trị động mạch |
| Liệu pháp nhiệt | Dụng cụ Coagulation grasper cm máu, đốt điện bằng sóng cao tần radiofrequency ablation, liệu pháp áp lạnh ryotherapy |
| Phương pháp cơ học | Hệ thống kẹp OTSC, khâu qua nội soi, kim bấm stapler dạng đường linh hoạt (đang thử nghiệm) |
| Các liệu pháp điều trị tại chỗ | Hemospray, endoclot, pure-Stat, nút máu ankaferd, cellulose bị oxy hóa |
Table 3 Summary of the pros and cons of emerging endoscopic modalities for the treatment of non-deforming gastrointestinal bleeding.




Over the past two decades, mortality and morbidity from variceal upper gastrointestinal bleeding have decreased sharply due to significant advances in therapeutic endoscopic therapy. The use of devices such as the bronchoscope clamp system, Coagrasper, Hemospray powder and laparoscopic suture has greatly evolved and expanded to achieve hemostasis as a primary method or when therapeutic devices Conventional methods such as thermal probes, endoclip hemostatic clips, or epinephrine injections do not control bleeding.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
References1. Alzoubaidi D, Lovat LB, Haidry R. Management of non-variceal upper gastrointestinal bleeding: where are we in 2018? Frontline Gastroenterol. 2019;10:35-42. [PubMed] [DOI]
2. Luo PJ, Lin XH, Lin CC, Luo JC, Hu HY, Ting PH, Hou MC. Risk factors for upper gastrointestinal bleeding among aspirin users: An old issue with new findings from a population-based cohort study. J Formos Med Assoc. 2019;118:939-944. [PubMed] [DOI]
3. Gralnek IM, Neeman Z, Strate LL. Acute Lower Gastrointestinal Bleeding. N Engl J Med. 2017;376:e50. [PubMed] [DOI]
4. Khamaysi I, Gralnek IM. Acute upper gastrointestinal bleeding (UGIB) - initial evaluation and management. Best Pract Res Clin Gastroenterol. 2013;27:633-638. [PubMed] [DOI]
5. Van Leerdam ME. Epidemiology of acute upper gastrointestinal bleeding. Best Pract Res Clin Gastroenterol. 2008;22:209-224. [PubMed] [DOI]
6. Maliha Naseer et al., Endoscopic advances in the management of non-variceal upper gastrointestinal bleeding: A review, World J Gastrointest Endosc. Jan 16, 2020; 12(1): 1-16