This is an automatically translated article.
Posted by Master, Doctor Mai Vien Phuong - Department of Examination & Internal Medicine - Vinmec Central Park International General Hospital
Esophageal cancer (EC) is the 10th most common cancer and the 8th leading cause of death worldwide with more than 80% of deaths in developing countries. The epidemiology of esophageal cancer has undergone a significant change worldwide over the past 30 years. Esophageal cancer mainly consists of two distinct histological subtypes: squamous cell carcinoma (ESCC) and adenocarcinoma (EAC).
1. Global epidemiological trends
Huge differences in incidence exist between Asian and Western populations, and between countries, up to 500 times and even within a particular country. The estimated worldwide incidence of esophageal cancer was 455,784 in 2012 with 400,156 deaths and is expected to be around 576,000 in 2015 with 486,000 deaths. The highest rates in both men and women were found in South and East Africa and East Asia with the lowest rates observed in West and Central America. West and Central Africa have very low rates, in stark contrast to East and South Africa. An esophageal cancer belt (esophageal cancer belt) with the highest incidence of squamous cell carcinoma in the world - Exists in an area extending from the border of the Caspian Sea and Turkey through the southern republics of the former Soviet Union and into northern China. Malawi has the highest morbidity and mortality rates in the world, followed by Turkmenistan. Among developed countries, Australia and New Zealand have the highest rates, followed by North America, Central and Eastern Europe.
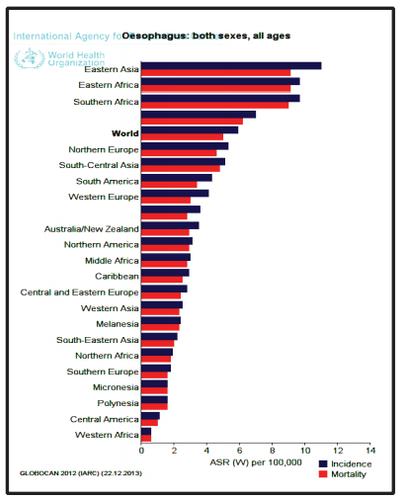
Tỉ lệ ung thư thực quản trên thế giới
The incidence as well as mortality has decreased significantly in China, Hong Kong, Japan, Korea and Singapore while it is increasing in Taiwan and Vietnam. Cixian County in China has one of the highest incidence rates in China and the world.
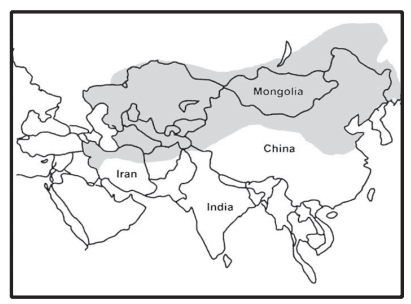
Vành đai ung thư thực quản ở châu Á
2. Epidemiological determinants
There are significant differences in the incidence of esophageal cancer based on sex, ethnicity, country of origin, dietary habits, and environmental factors.
Gender
In the West, men develop squamous cell carcinoma three to four times more often and adenocarcinoma six to eight times more often than women. Interestingly, the male-female incidence (IRR) of squamous cell carcinoma in all ages and particularly in the >70 age group was significantly reduced. The sex ratio decreased steadily and significantly with increasing age of adenocarcinoma, unrelated to menopause. The prevalence of the disease in women is 5.1 times higher than in men in the United States. The rapid increase in esophageal cancer, which currently ranks in the top 10 in incidence from 1975-2004, is due to a greater increase in male rates than female rates, although adenocarcinoma is rapidly increasing in skin women. white similar to white males. The highest mortality rates for both sexes are in East and South Africa, and East Asia. South Asian women are at higher risk than men with a six-fold risk difference between Pakistani and Bangladeshi women, while there is no gender difference in black or Chinese populations.
Role of the hormone estrogen
The pathogenesis of a higher incidence of esophageal cancer in men is speculative. For risk factors such as estrogen exposure, BMI and H.pylori infection, there was no evidence of causing a gender imbalance. Estrogen in women as a protective factor has long been recognized without convincing data. Studies on hormone replacement therapy, including estrogen therapy, and fertility, do not support the estrogen theory, although breastfeeding is thought to have a protective effect. Estrogen receptors in esophageal tissue have been identified, and in vitro studies indicate that estrogen can inhibit esophageal carcinogenesis. Erosive reflux esophagitis (GERD) may be more common in younger men than in women. Other differences between the sexes that may account for the higher incidence of adenocarcinoma include android obesity (abdominal obesity or metabolic obesity) and GERD predisposing factors. Epidemiological differences in the incidence of premalignant lesions between both sexes are detailed below Barrett's esophagus.
3. Esophageal squamous cell cancer
Currently, squamous cell carcinoma is mainly a disease of developing countries (90% of esophageal cancers) with the majority of cases belonging to the cancer group. There are also areas of high incidence of squamous cell carcinoma in industrialized countries, including northwestern France, Iceland, Scotland and Finland. In the UK, Bangladeshis are six times more likely to develop squamous cell carcinoma than Pakistanis.
Ung thư tế bào vảy thực quản chiếm tỉ lệ cao ở các quốc gia có nền công nghiệp phát triển
The incidence of squamous cell carcinoma is higher in men than in women and higher in black men than in white men. Higher BMI, in sharp contrast to adenocarcinoma, is considered a protective factor for squamous cell carcinoma. Red meat, lamb and boiled meat and higher drinking temperatures were found to be associated with an increased risk of squamous cell carcinoma, while fruits and vegetables, white meat, poultry, fish and liver were preserved. defense for unclear reasons. Hot foods and drinks contaminated with fungi, containing various nitrosamines, spicy foods, deficiency of β-carotene, vitamins A, C and E and the minerals zinc, selenium and molybdenum are risk factors for cancer esophagus has been studied. Neuroblastoma, a rare disorder involving hyperkeratosis of the palms and soles, is associated with a high incidence of squamous cell carcinoma.
In the United States, the incidence is higher in coastal South Carolina and the Washington DC/Baltimore metropolitan area than in other states. Smoking and alcohol consumption are the major known risk factors for squamous cell carcinoma in the United States, accounting for more than 90% of cases in men and, to a lesser extent, the cancer. glandular epithelium.
4. Acetaldehyde and esophageal cancer
Acetaldehyde, the main metabolite of ethanol, forms additives with DNA and this additive is responsible for the carcinogenic effects of alcoholic beverages. Patients with squamous cell carcinoma, particularly alcoholics, current smokers, and those with the ALDh3-2 allele and multiple Lugol-iodine-stained lesions at endoscopy, are at increased risk for cancer. squamous cell epithelium of the head and neck. A history of oral lye ingestion is well known to cause stenosis and squamous cell carcinoma with rates varying from 2.6 to 7.2% in cases of tracheal separation. . The incidence of esophageal cancer after drinking lye is 1000 to 3000 times increased with a latency period of up to 60 years.
Currently, Vinmec International General Hospital has implemented a package of screening and early detection of gastrointestinal cancers (esophagus - stomach - colon) Package of screening and early detection of gastrointestinal cancers (practice) esophagus - stomach - colon) of Vinmec combines clinical and paraclinical examination to bring about the most accurate results possible. Specifically, Vinmec's package of screening and early detection of gastrointestinal cancers (esophagus - stomach - colon) includes:
Gastroenterology specialist examination (by appointment) Gastroscopy and colonoscopy with NBI endoscope with anesthesia Gastroscopy and colonoscopy with anesthesia (Drugs) Gastroscopy and colonoscopy with anesthesia (VTTH) Routine histopathological examination fixed, transferred, cast , cut, stain... biopsies (upper gastrointestinal tract (esophagus, stomach, duodenum, papilla) through endoscopy Routine histopathological examination is fixed, transferred, cast, cut, stained. ..biopsy specimens (lower gastrointestinal tract through endoscopy (colon, rectum)
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
References
Janeesh sekkath veedu , changing epidemiology of esophageal cancers worldwide – what do we learn? Epidemiology of gastrointestinal cancers,
2, practicalgastro, january 2014 • volume XXXVIII, issue 1. Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. Mar-Apr 2005;55(2):74-108. Stavrou EP, McElroy HJ, Baker DF, Smith G, Bishop JF. Adenocarcinoma of the oesophagus: incidence and survival rates in New South Wales, 1972-2005. Med J Aust. Sep 21 2009;191(6):310-314.