This is an automatically translated article.
The article was written by Specialist Doctor II Nguyen Bang Phong - Deputy Head of Cardiology Department - Vinmec Times City International HospitalSyncope is a temporary loss of consciousness due to total cerebral hypoperfusion with the following features: rapid onset, short duration, complete recovery. Although completely self-healing, in many cases, fainting causes serious consequences such as injury, especially when operating a motor vehicle, while climbing, when alone (in the toilet, etc.) .
1. Causes of Fainting
Syncope is divided into 2 main types: cardiac syncope and non-cardiac syncope.
1.1 Fainting due to heart disease
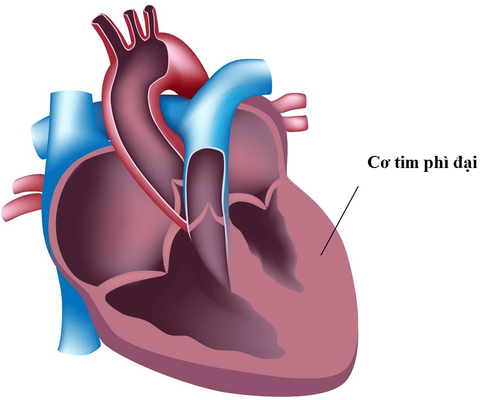
When a patient has syncope, especially when syncope recurs many times, the doctor will conduct a medical examination, clinical examination and additional techniques such as: electrocardiogram, Holter electrocardiogram, echocardiogram, etc. stress electrocardiogram, stress echocardiogram, coronary angiography, cardiac electrophysiological probe, remote heart rate monitoring device to detect heart disease: structural heart disease, heart failure, coronary artery disease , arrhythmia. Syncope due to heart disease often has a poor prognosis.
Ngất do bệnh tim
1.2. Fainting is not due to heart disease
After ruling out heart disease, the doctor will conclude that the syncope is not due to heart disease. Syncope that is not due to cardiac disease usually has a better prognosis, unless trauma from a fall during syncope. Non-cardiac syncope includes: orthostatic hypotension, syncope due to carotid sinus reflex, syncope due to vagal reflex, syncope of unknown cause.
Syncope due to hypotension in standing position often occurs in the elderly. Low blood pressure can be caused by an overdose of antihypertensive drugs, by not drinking enough water, by diarrhea, by autonomic nervous system failure, by standing for a long time.
Reflex syncope often occurs in young people, often with motivating factors such as: emotions, pain, fear (fear of blood, fear of surgery...), unpleasant taste, horror scene, urination , swallowing quickly, dodging, coughing, sneezing, after exertion, laughing a lot, stuffy crowd, hot and cold, collar or tie too tight. Reflex syncope often has bradycardia, even asystole, for a short period of time. Before syncope due to reflex, there are usually aura: pallor, sweating, nausea - vomiting.
Other causes: In some cases of syncope not due to heart disease, the usual examination cannot determine whether it is reflex syncope or orthostatic hypotension. Some cases of loss of consciousness but not yet identified as syncope or other causes such as epilepsy, pseudosyncope due to psychological disorders (Histeria).
During the examination, doctors often apply techniques such as carotid sinus massage, active standing test, deep breathing test, Valsalva test and especially the tilt table test to contribute to the diagnosis of the cause. This is a fairly simple technique, easy to perform and safe, contributing quite effectively in identifying syncope due to hypotension in standing or due to reflex, or distinguishing syncope from epilepsy, pseudosyncope due to hypotension. mentality.
2. Tilt table test
2.1 What is the tilt table test?

Nghiệm pháp bàn nghiêng
In an upright or leaning position, blood tends to pool in the legs, which more or less makes the blood flow to the heart and then to the brain to decrease. Normally, the body responds to autonomic responses with a slight increase in blood pressure (autonomic) and heart rate (vagal reflex). If the autonomic nerve is impaired, the blood pressure not only does not increase but also decreases, causing fainting due to a drop in blood pressure in the standing position (orthostatic hypotension). If the autonomic reflex is disturbed, the heart rate not only does not increase but on the contrary also decreases, even asystole for a short time, then syncope occurs, called vasovagal syncope. . Some cases of neuro-responsive disorder are characterized by an excessive increase in heart rate, often increasing by 30 beats/min or more, called postural reflex tachycardia syndrome (PoTS). .
On that basis, cases of syncope, especially multiple syncope, were identified as syncope not due to heart disease, cases needing to distinguish syncope or epilepsy, pseudosyncope due to psychological disorder, If the cause is unidentified or repeated multiple falls, a tilt table test (NPBN) is indicated.
2.2 Procedure for performing tilt table test
The tilt table test is conducted in a quiet, temperature-stable room with an oxygen supply, suction head, blood pressure monitor and electrocardiogram, electrocardiogram recorder, emergency equipment and medications.
Before performing the tilt table test, the patient should be thoroughly explained about the principle, procedure and possible response scenarios for the best coordination. Patients should fast for 4 hours before the procedure to avoid choking on food or water when fainting.
The patient is placed supine on a table that can be raised about 60 -70° and rapidly lowered to a horizontal position in 10 seconds. Secure straps at the knee, at the hip and at shoulder level. Place an intravenous line through which to administer medication if needed.
Pre-test phase: Patient in supine position, monitor - record systolic blood pressure (BP) and heart rate every 2 minutes for 6 minutes. (Currently, a continuous blood pressure monitoring system with finger cuffs has just appeared: beat to beat blood pressure)
Passive phase (20 minutes): Set up a 70° sloping table, monitor - record blood systolic pressure, heart rate every 1 minute. Note the prodromals: pallor, sweating, nausea-vomiting. When syncope occurs, quickly lower the table to 0° and the patient also recovers quickly, possibly with slight fatigue. Need to continue monitoring heart rate, blood pressure, vomiting, dizziness for another 15 minutes. If monitoring for 20 minutes does not occur, switch to drug phase.
Mixing medicine (15 minutes): Table remains in a 70° incline position. Spray 1 dose of Nitroglycerine 0.4 mg under the tongue. Continue monitoring - record systolic blood pressure, heart rate every 1 minute. Note the prodromals: pallor, sweating, nausea-vomiting. When syncope occurs, quickly lower the table to 0° and the patient also recovers quickly, possibly with slight fatigue. Need to continue monitoring heart rate, blood pressure, vomiting, dizziness for another 15 minutes. If follow-up for 15 minutes does not occur, the test is terminated.
2.3 Result scenarios of tilt table test
No syncope, usually little change in systolic blood pressure and heart rate: negative tilt table test.
There is no syncope, systolic blood pressure and heart rate are little changed, but there are some symptoms: dizziness, headache, palpitations, shortness of breath... and then fainting: Psychogenic syncope.
Syncope with a rapid decrease in heart rate and systolic blood pressure and a rapid return to normal when lying horizontally: syncope due to vagal syncope.
Syncope occurs soon after a few minutes of tilting the table, accompanied by a rapid decrease in systolic blood pressure with syncope and a rapid return to normal when lying horizontally; little change in heart rate: Syncope due to hypotension in standing position.
Increased tachycardia at least 30 beats/min (additional 40 beats/min in people < 19 years), little change in blood pressure, with or without symptoms: standing tachycardia (PoTS).
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.