This is an automatically translated article.
The article was professionally consulted with Specialist Doctor II Cao Thi Thanh - Pediatrician - Pediatrics - Neonatology - Vinmec Hai Phong International General Hospital.Neonatal necrotizing enterocolitis is one of the most common gastrointestinal emergencies. This is a disorder characterized by ischemic necrosis of the intestinal mucosa. Despite the many means of early recognition and aggressive treatment, infants with inflammatory bowel disease still have significant long-term morbidity in neonatal intensive care survivors, especially in infants. premature birth or low birth weight.
1. What are the signs of necrotizing enterocolitis in infants?
The clinical presentation of necrotizing enterocolitis in the neonate was nonspecific in the history, and included vomiting, diarrhea, food intolerance, and high gastric residue after eating. More specific symptoms of acute enterocolitis in infants are bloating and fishy-smelling stools or blood in the stool.As the infant develops enteritis, he or she will have increasing abdominal pain accompanied by edema of the abdominal wall, abdominal distension, or palpation of bowel loops indicating a fixed and dilated loop. The systemic signs of necrotizing enterocolitis in the neonate may include lethargy or slow breathing, respiratory arrest, bradycardia, coma, temperature instability, hypoglycemia, and shock. These are signs that the child has fallen into a critical condition.
Epidemiological studies have demonstrated that the signs of necrotizing enterocolitis in neonates are significantly different in term and preterm infants. Specifically:
For full-term infants Compared with premature infants, term infants with necrotizing enterocolitis usually have early onset with a reported mean age of onset 1-3 days after birth. However, some cases can appear as late as 1 month of age.
Newborns with necrotizing enterocolitis immediately after birth often have other medical conditions, such as asphyxia at birth, respiratory failure, congenital heart disease or metabolic abnormalities, and a morphological history. abnormal development of the fetus.
In addition, maternal risk factors that decrease fetal intestinal blood flow, such as placental insufficiency due to acute illness (eg, pregnancy-induced hypertension), chronic disease (eg. diabetes) or maternal cocaine abuse may also increase the risk of neonatal necrotizing enterocolitis.
Signs and symptoms of necrotizing enterocolitis in neonates are found when the child vomits repeatedly or has gastric fluid, abdominal distention, bloody stools, abdominal X-ray shows dilated bowel loops , intestinal pneumothorax, presence of air in the abdomen, and other signs of systemic infection, including shock and metabolic acidosis.
Acute enteritis in premature infants The risk of acute enteritis in preterm infants occurs within a few weeks of birth, later than in term infants.
Premature infants with a patent ductus arteriosus are at increased risk for co-morbidity with necrotizing enterocolitis in the neonate, especially if they are treated with indomethacin to close the ductus arteriosus. However, infants with persistent ductus arteriosus, which required surgical ligation, were found to have higher rates of neonatal necrotizing enterocolitis-related mortality than those with established ductus arteriosus. was successfully closed without surgery.
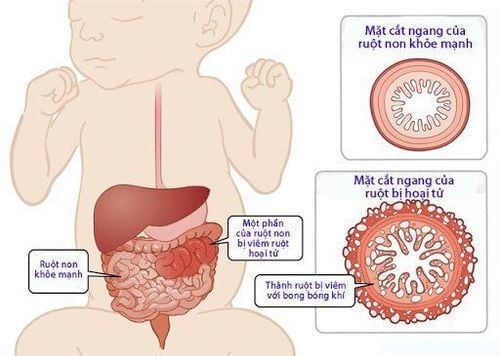
Hình ảnh mô tả viêm ruột hoại tử ở trẻ sơ sinh
2. Examination and diagnosis of necrotizing enterocolitis in neonates
The findings on physical examination to diagnose necrotizing enterocolitis in neonates may be primarily gastrointestinal, including any one or all of the following:Increased abdominal size (abdominal distension) ); Loops of bowel are visible on the abdominal wall; Visible abdominal distension and decreased bowel sounds; Change in stool properties; Hematuria; An intra-abdominal mass may be palpable; Erythema on the abdominal wall; Systemic signs pointing to the possibility of acute enteritis in the neonate may include any of the following:
Respiratory distress; Decreased peripheral perfusion; Circulatory shaft. When the neonate has new-onset inflammatory bowel disease, the clinical signs may be mild and insidious, while the infant is in an advanced stage, clinical abnormalities often begin to be severe and severe.

Viêm ruột hoại tử ở trẻ sơ sinh có thể thăm khám lâm sàng khi thấy vòng bụng to hơn
3. Tests to diagnose necrotizing enterocolitis in neonates
The initial presentation of necrotizing enterocolitis in neonates often includes nonspecific signs of food intolerance, such as gastric residue, abdominal distension, or bloody stools. Abdominal imaging studies are important at this stage. In fact, an abdominal radiograph should be performed if there is any doubt about the possibility that the infant has enteritis.Besides, other tests are also needed if the child is showing any systemic signs. The results will provide evidence of the severity of the disease and may assist in the direction of appropriate treatment. Such tests include:
Complete blood count: Complete blood cell count to evaluate white blood cell count, hematocrit, and platelet count is usually repeated at least every 6 hours if the clinical condition of the patient is Infants with inflammatory bowel disease continue to worsen. In addition, premature babies are prone to iron deficiency anemia. However, progressive hemolytic or coagulopathy blood loss in neonates with inflammatory bowel disease may manifest as acute hematocrit. On the other hand, a decreased platelet count in the complete blood count also indicates acute necrotizing enterocolitis in the neonate. In addition, thrombocytopenia can be exacerbated in cases where the child has complications of coagulopathy or reactions to gram-negative organisms and endotoxins. Blood cultures: Blood cultures should be obtained prior to initiating antibiotics in any patient presenting with any signs or symptoms of sepsis or the possibility of enteritis. Although blood culture is usually negative in most cases of necrotizing enterocolitis in neonates, it is also a criterion for differential diagnosis. Furthermore, the results of identifying specific microbial agents will be valuable in guiding antibiotic therapy. Serum electrolytes: Serum electrolytes may show some characteristic abnormalities in the setting of necrotizing enterocolitis in neonates, including: hyponatremia, metabolic acidosis. Abdominal ultrasonography: Abdominal ultrasound may be helpful when necrotizing enterocolitis in neonates is suspected. However, neonates with severe enteritis and large amounts of intra-abdominal air interfere with the evaluation of intra-abdominal structures by ultrasound. However, ultrasonography is excellent for identifying and quantifying intraperitoneal fluid or ascites. Continuous ultrasound examination helps to monitor the progression of ascites as a marker for the course of the infant with inflammatory bowel disease. Upper GI Endoscopy: Upper gastrointestinal endoscopy usually does not or only evaluates part of the small intestine. It is not instrumental in diagnosing necrotizing enterocolitis in infants but helps to find the cause if the child is experiencing vomiting, bloating, or other gastrointestinal abnormalities.
4. Diagnosis of necrotizing enterocolitis in neonates by invasive measures
Ascites for testing may be needed during the diagnosis of advanced necrotizing enterocolitis. This procedure is performed most safely by performing it under ultrasound guidance. A positive free-flow peritoneal puncture of at least 0.5 mL of bacterial brown fluid on Gram stain is very specific for necrotizing enterocolitis.In addition, neonatal necrotizing enterocolitis most commonly affects the terminal ileum and proximal ascending colon. At this point, the anatomical diagnostic evidence is intermittent mucosal lesions, including coagulative necrosis of the mucosa with active and chronic inflammation, mucosal ulceration, edema, hemorrhage, and edema. pneumothorax of the submucosa.
Newborns with advanced enteritis can lead to necrosis of the entire intestinal wall. The regenerative changes with epithelial neoplasia, granulomatous formation, and fibrosis are the pathological evidence for the definitive diagnosis of necrotizing enterocolitis in neonates.
In summary, neonatal necrotizing enterocolitis usually occurs during the second to third week in premature, formula-fed infants. In the cases of infants with enteritis, the common initial manifestations are digestive disorders, abdominal distention, vomiting, delayed digestion and bloody stools. Early diagnosis of acute enterocolitis in neonates and sometimes the need for surgery to remove the damaged bowel in time can significantly improve the prognosis.

Chọc dịch cổ trướng để xét nghiệm giúp chẩn đoán viêm ruột hoại tử ở trẻ sơ sinh
Gathering a team of leading pediatricians: including leading experts with high professional qualifications ( professor, associate professor, doctorate, master), experienced, worked at major hospitals such as Bach Mai, 108... The doctors are well-trained, professional, conscientious - understanding and understanding young psychology. Besides domestic pediatricians, the Department of Pediatrics also has the participation of foreign experts (Japan, Singapore, Australia, USA) who are always pioneers in applying the latest and most effective treatment regimens. . Comprehensive services: In the field of Pediatrics, Vinmec provides a series of continuous medical examination and treatment services from Newborn to Pediatric and Vaccine,... according to international standards to help parents take care of their baby's health from birth to childhood. upon reaching adulthood. Advanced techniques: Vinmec has successfully deployed many specialized techniques to make the treatment of difficult diseases in Pediatrics more effective: neurosurgery - skull surgery, hematopoietic stem cell transplantation in cancer treatment. Professional care: In addition to understanding children's psychology, Vinmec also pays special attention to the children's play space, helping them to play comfortably and get used to the hospital's environment, cooperate in treatment, improve the efficiency of medical treatment.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
References: uptodate.com, my.clevelandclinic.org, emedicine.medscape.com