This is an automatically translated article.
The article was written by a doctor of Laboratory Department - Vinmec Ha Long International General Hospital.1. Physiological functions of the liver
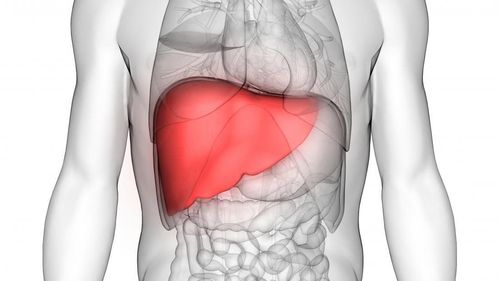
The liver performs important functions, including: metabolism, excretion and detoxification
1.1. Metabolic function Glucose metabolism The liver plays a role in regulating blood sugar of the body: The liver is the body's store of glucose in the form of glycogen. Thanks to the rich enzyme system, the liver synthesizes glycogen from simple sugars (glucose, galactose, fructose, manose), from intermediate metabolic products (lactate, pyruvate, acetyl CoA,...). When the concentration of these substances in the blood increases, the liver will synthesize glycogen for storage. When blood glucose tends to fall below normal, the liver will increase the breakdown of glycogen to create glucose into the blood. Muscles and some other organs in the body also contain glycogen but cannot be broken down to form glucose (because only the liver has the enzyme Glucose-6-phosphatase). The liver also synthesizes heparin (a natural coagulant of polysaccharide nature), converts glucose into glucuronic acid (essential component for the liver's detoxification function. In the intestines (as constituents, such as glycerol, fatty acids/emulsions), only a small part is resynthesized into lipids in the intestine, and most is transported to the liver before transport. In addition to synthesizing neutral lipids and cholesterol, the liver also synthesizes a lot of phospholipids (which are polar lipid molecules that play a major role in the structure of serum lipoproteins).

Gan đảm nhận chức năng chuyển hóa, bài tiết và khử độc cho cơ thể
Lipid degradation occurs strongly in the liver, producing fragments of acetyl CoA. Then a part of acetyl CoA is "burned" in the liver to provide energy for the liver to function, a part is used by the liver to synthesize cholesterol and bile acids, most of which is further synthesized by the liver into ketones and put into the blood. to other organisations. In these tissues, ketones are converted back to acetyl CoA for burning to provide energy for the activities of that tissue. From this activity, the liver oxidizes fatty acids "for" other organs/organs/tissues of the body. Protein metabolism The liver synthesizes all albumin and part of serum globulins, fibrinogen, ferritin, prothrombin and most other plasma proteins. When liver function is impaired, blood albumin decreases, the albumin/globulin (A/G) ratio decreases and there are coagulation disorders. The liver contains many enzymes involved in amino acid degradation, especially transaminases (AST/GOT, ALT/GPT). When the liver is damaged, transaminases are released and are elevated in the serum, while cell damage is deeper, releasing some enzymes that are only distributed in the mitochondria (such as GLDH). The liver is the only site to synthesize urea from NH3 (product of amino acid degradation) this function is very active, even if 3⁄4 tissues of the liver are destroyed or removed, the function of urea synthesis liver remains normal. The liver participates in the degradation of hemoglobin, produces free bilirubin (indirect bilirubin) and especially conjugated bilirubin (direct bilirubin) – also known as bile pigment, water soluble and excreted in the bile. or urine. 1.2. Excretory function The liver produces and excretes substances of intracellular and extracellular origin into the biliary tract and urine. The liver produces about 3 liters of bile per day and excretes an average of 1 liter per day in adults.
1.3. Detoxification function Endogenous toxins (products of metabolism of substances such as H2O2, free bilirubin, NH3, ..) or exogenous (introduced from the outside into the body such as alcohol, antibiotics, sleeping pills, etc.) .) are retained by the liver, converted into non-toxic substances and excreted in the following two ways:
Fixed elimination: toxic substances, when reaching the liver, are retained and then excreted unchanged in the biliary tract. Toxins eliminated in this way include heavy metal salts (Cu salts, Pb salts, etc.) and some pigments. Chemical mechanism: is the main and important detoxification of the liver. Toxic substances are converted into non-toxic substances that are easily soluble in water to be eliminated.
Gan chuyển các chất độc thành chất không độc và đào thải ra bên ngoài
2. Liver function tests
2.1. Test to assess liver cell damage and destruction Measuring transaminase enzyme activity (AST/GOT, ALT/GPT): AST/GOT is widely distributed in body tissues, abundant in liver, heart and muscle skeletal. ALT/GPT is mainly distributed in the liver, to a lesser extent in the kidney and skeletal muscle. In hepatitis, or other injuries such as trauma, biliary obstruction, liver cancer, these two enzymes are increased, the degree of increase in each disease is different.Measure GGT (γ-glutamyltransferase) activity: GGT is an enzyme that binds to cell membranes. Abundant in liver, kidney and pancreas. In hepatobiliary disease, GGT is elevated in biliary obstruction, liver damage due to intoxication by various causes (such as alcohol intoxication, CCl4, halothan...). In some cases of hepatobiliary disease without jaundice, an increase in GGT and ALP enzyme activity is indicative of liver disease. Measurement of LDH (Lactate dehydrogenase) activity: LDH is present in the cytoplasm of all cells of most tissues in the body, an increase in LDH activity is valuable for reporting damage to certain tissues in the body. . When LDH is elevated, further analysis of isozymes will indicate the origin of LDH, for example in liver disease (such as liver cancer) will see an elevated LDH5. Measurement of GLDH (Glutamate dehydrogenase) activity: GLDH is present in the mitochondria of hepatocytes. When the degree of liver damage is severe and deep, GLDH will be elevated in plasma. Measurement of 5' Nucleotidase activity (5NT): 5'NT is present in most tissues, but not in bone, thus helping to determine whether elevated ALP is due to liver or bone or other conditions Physiological such as growing children or pregnant women. In bone disease, ALP is increased but 5'NT is not. 2.2. Test to evaluate biliary obstruction Measure ALP (Alkaline phosphate) or alkaline Phosphatase activity: ALP originates mainly in bone (forming osteoblasts), a small part in liver microsomes, placenta. In hepatobiliary disease: mild to moderate increase in ALP in people with hepatitis, cirrhosis; increased sharply when biliary obstruction due to extrahepatic causes (biliary obstruction due to biliary stones, primary biliary cirrhosis); always increased in metastatic liver disease.

Đo hoạt độ ALP để phát hiện và đánh giá tình trạng tắc mật
Quantification of Bilirubin (hereinafter abbreviated as Bil, including Total Bil, Free Bil / Indirect Bil, Direct Bil / Conjugated BIL). + When total Bil concentration increases, the specific determination of increased Bil indirectly or increased directly Bil is very useful for classifying the increase in plasma Bil:
Increase in direct Bil: when >50% of the amount of Bil plasma (Bil TP) is direct Bil,
Indirect Bil increase: when >80% of plasma Bil (Bil TP) is indirect Bil,
+ Increase in Bil is common in hepatobiliary disease due to hepatitis or obstruction , or extrahepatobiliary disease such as hemolytic disease (hemolysis)
Urobilinogen test in stool and urine: Urobilinogen is colorless, a product of bilirubin metabolism in the intestinal lumen. Normally about 90% of urobilinogen is converted to stercobilinogen, stercobilin and excreted in the feces (fecal pigment), the rest is reabsorbed to the liver via the portal vein and excreted by the kidneys. Urobilinogen is increased in urine in hemolytic disease, hepatitis,
In biliary obstruction: complete biliary obstruction without urobilinogen in feces and urine.
Bilirubin in the urine (in the urinalysis test) + Hemolytic jaundice (Jaundice of pre-hepatic causes - increased indirect bilirubin in the blood): no bilirubin in the urine (due to the insoluble indirect bilirubin). in water, not filtered by the kidneys).
+ The cases of hepatobiliary disease causing direct increase in Bil, there is Bil in the urine.
2.3. Test to evaluate synthesis function Quantitative blood albumin: The liver synthesizes all albumin in serum. However, the nutritional status is important, because the raw materials for the liver to synthesize albumin are amino acids that are supplied mainly from food sources into the body, especially tryptophan. Some diseases that cause albumin loss also affect albumin levels (eg, glomerular damage causes loss of albumin in the urine, burns cause albumin loss, ...).

Định lượng albumin trong huyết thanh để đánh giá chức năng tổng hợp của gan
In impaired liver function, serum albumin concentration will decrease and decrease in albumin concentration will not be immediately apparent (due to albumin half-life/half-life of 20 days), decrease in albumin concentration due to Impaired liver function is usually detected about 30 days after the onset of the disease. As such, serum albumin is more important in assessing chronic liver disease than in acute conditions, which should be kept in mind when evaluating test results.
Quantification of Total Protein: The liver is the major source of most serum proteins (albumin, fibrinogen and other clotting factors, most alpha and beta globulins). In liver failure, the total protein concentration decreases, the A/G ratio decreases. Measurement of Cholinesterase activity decreases with liver failure. Quantification of coagulation factors fibrinogen, prothrombin decreased in liver failure Quantitative ammonia (NH3): increase when liver function is severe, patients may be in a pre-coma/hepatic coma. 2.4. Test to evaluate the function of detoxification BSP excretion test (Bromosulfophthalein) The basis of the test is based on the liver's function to capture pigments in blood plasma and release into bile: when injected into the body a quantity of BSP pigments. After a certain time, the amount of BSP will gradually decrease in the blood. As liver function declines, the ability to capture pigments for elimination is reduced.
Currently, Vinmec International General Hospital is implementing a hepatobiliary screening package that includes all tests to evaluate liver function, bringing peace of mind and accurate results to customers. When there are signs of liver disorders or a history of hepatobiliary disease or even if there are no symptoms, proactive liver function tests are necessary to protect your health.
If you have a need for consultation and examination at Vinmec Hospitals under the national health system, please book an appointment on the website for service.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.