This is an automatically translated article.
Congenital duodenal obstruction is a rare disease that occurs more often in boys than in girls. In order to remove the obstruction, to establish the gastrointestinal tract, the child should be operated on to treat the ileus.
1. What is duodenal obstruction?
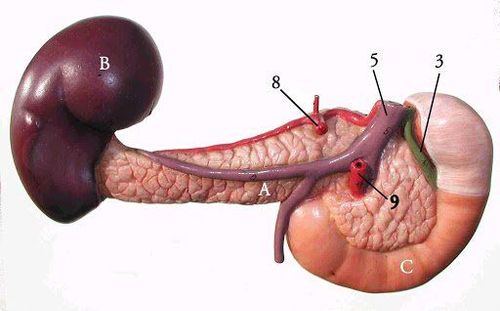
Congenital duodenal obstruction is a rare disease, with an incidence of 1/5000-1/10,000 births, occurring more in boys than in girls. Duodenal obstruction may be caused by duodenal atresia, duodenal stenosis, cricoid pancreatitis, volvulus, or incomplete rotation of the bowel. Other possible causes are portal vein anterior duodenum, superior mesenteric artery syndrome. There is a high percentage of children with duodenal obstruction associated with other congenital malformations such as Down syndrome, congenital heart disease, esophageal atrophy, urinary tract malformation...
When duodenal obstruction is present, children often have clinical symptoms such as:
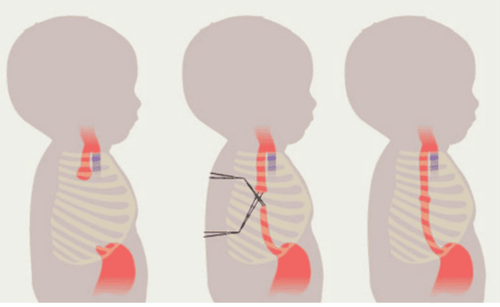
Jaundice , upper abdomen distention, sometimes see gastric increased peristalsis, lower abdomen collapsing Vomiting profusely and continuously, vomiting yellow or green milky or bile fluid Signs of combined malformations such as Down syndrome, cardiac malformation, anorectal malformation, esophageal atrophy... Diagnosis of duodenal obstruction is confirmed when performing abdominal X-ray and ultrasound with bubble image. twins in the womb.
Treatment of duodenal obstruction in children by surgery to remove the obstruction, establish gastrointestinal circulation. However, this is not an emergency surgery, so it is possible to fully compensate and correct the electrolyte imbalance in the few days before surgery.
2. In which cases does laparoscopic surgery treat duodenal obstruction?
Laparoscopic duodenal obstruction surgery is indicated in children with duodenal atresia, duodenal obstruction due to ring pancreas, anterior portal vein of duodenum. General requirements are children weighing 1500g or more, stable condition, no mechanical ventilation, no vasopressor, no sepsis and no abnormalities affecting laparoscopic surgery.
Laparoscopic surgery for duodenal obstruction is not performed in children with contraindications to surgery; Children weighing less than 1500g, respiratory failure, circulatory failure, sepsis, blood clotting disorders, severe congenital heart defects. This technique is also not performed with children with co-morbid abnormalities affecting laparoscopic surgery such as other accompanying intestinal atrophy, esophageal atrophy requiring gastric bypass, children without anus, ...

Để điều trị tắc tá tràng nội soi, trẻ cần đảm bảo một số yêu cầu chung
3. Preparing for duodenal obstruction surgery by laparoscopic method
The team performing laparoscopic surgery for duodenal obstruction in children includes 1 main surgeon, 1 auxiliary surgeon, 1 instrument. Equipment needed includes: laparoscopic surgery system, trocars of suitable sizes, pins, suction tubes, needle clamps,...
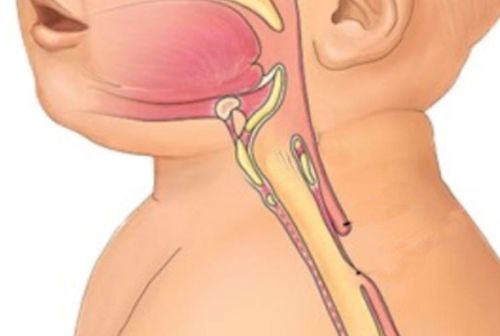
Before performing duodenal obstruction surgery, the doctor will re-examine to check Check the child's condition, detect accompanying abnormalities. Indications for tests such as blood clotting function tests, electrolytes, bilirubin, ... The team placed gastric tube, urinary catheter and gave the child prophylactic antibiotics to prevent infection during surgery.
4. Steps to perform laparoscopic surgery to treat duodenal obstruction in children
Newborn patient is placed supine, position across the operating table. Older patients will be placed vertically at the end of the table, feet lower than the abdomen. The surgeon stands in the middle of the patient's legs, the monitor is placed on the patient's head. The assistant holding the camera stood to the right of the surgeon.
The surgical team placed trocars and inflated the abdomen, maintaining intra-abdominal pressure from 7-9 mmHg with a flow rate of 2-3l/min depending on age.
The stages of laparoscopic surgery to treat duodenal obstruction take place as follows:
Laparoscopy to diagnose the cause of duodenal obstruction. Suture the round ligament of the liver to the anterior abdominal wall to lift the liver. Release the duodenum D1-D3, and clearly see the small narrowing below the obstruction to identify the obstruction above it. Sew the PDS 5.0 thread together above and below the occlusion, and then hang it on the anterior abdominal wall. Open below the clog (vertically) and above the clog (diagonally) down 10-15mm. Suture the anastomosis of the posterior duodenum, starting from close to the suture of the duodenum with a loose stitch PDS 5.0. Suture the anterior wall of the duodenum, from top to bottom, with a separate stitch PDS 5.0. After suturing the anastomosis, cut the duodenal suspensory thread Carry out abdominal washing, withdraw the trocars and suture the incisions

Mổ nội soi điều trị tắc tá tràng ở trẻ cần được thực hiện bởi một Ê-kíp mổ
5. Follow-up after laparoscopic surgery
After surgery for duodenal obstruction, the child fasted and received intravenous nutrition for 3-5 days or longer. Usually 3-4 days after surgery, when the gastric tube shows clear fluid, start feeding the child and gradually reduce the amount of fluid. Closely monitor the child's general condition and abdomen to detect infection, peritonitis.
Some common complications when laparoscopic surgery to treat duodenal obstruction are:
Tear of duodenal wall, liver damage due to endoscopic puncture. This complication is common during surgery in low birth weight infants due to the narrow surgical field. The surgical team will handle it based on the specific condition of the child. Leaky anastomosis: when detected, it must be re-operated as soon as possible to redo the anastomosis. Narrow anastomosis: perform gastrointestinal endoscopy to widen the anastomosis, if there are no results, re-surgery is required to redo the anastomosis. Laparoscopic duodenal obstruction surgery is indicated in children with duodenal atresia, duodenal obstruction due to ring pancreas, anterior portal vein of duodenum.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.