This is an automatically translated article.
The article is professionally consulted by - Master, Resident, Specialist I Trinh Le Hong Minh - Department of Diagnostic Imaging - Vinmec Central Park International General Hospital.
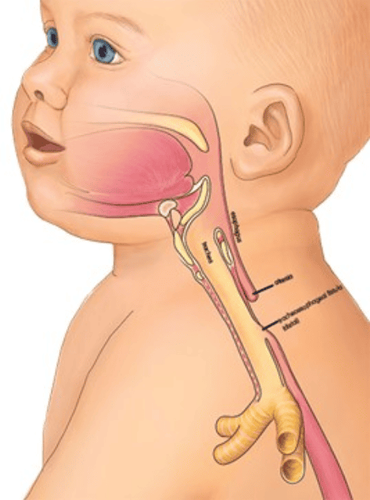
Congenital esophageal atresia is when one part of the esophagus in a child splits into two separate, unconnected parts. Therefore, children with this birth defect cannot transfer food from the mouth to the stomach, affecting the ability to breathe, surgical intervention should be carried out as soon as possible.
1. What is congenital esophageal atrophy?
Neonatal esophageal atrophy is a rare birth defect in which the esophagus grows into two separate and unconnected segments. Even in some children, the missing portion of the esophagus is very long and difficult to correct the connection with surgery alone.
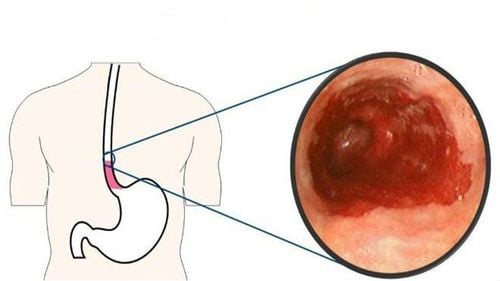
Consequences of congenital esophageal atrophy are that the esophagus is completely dysfunctional and the child cannot receive enough nutrition by mouth. In addition, babies are also very susceptible to respiratory infections such as pneumonia, conditions such as acid reflux.
Fortunately, congenital esophageal atresia can often be completely treated with surgery and children can still develop normally as children of the same age.
Teo thực quản bẩm sinh khiến trẻ không thể nhận đủ dinh dưỡng bằng đường miệng
2. What are the causes of congenital esophageal atresia?
The exact cause of congenital esophageal atrophy is not well understood but several factors appear to be related to genetics. The fact is that up to half of babies born with congenital esophageal atresia have one or more other birth defects, such as:
Trisomy 13, 18 or 21 gastrointestinal problems others, such as duodenal obstruction, enteritis, or incomplete anal plasty horseshoe kidney or polycystic kidney Musculoskeletal problems such as split spine

Teo thực quản bẩm sinh có liên quan đến yếu tố di truyền
3. How to diagnose congenital esophageal atresia?
The first signs of congenital esophageal atresia are usually detected very clearly soon after the baby is born, the most common are:
There is white foam in the baby's mouth that comes out continuously Continuous saliva flow Totally unable to suckle, swallow Frequent spitting up Cough or difficulty breathing, intense fussiness during feeding Pale skin color while feeding At this time, the doctor's immediate indication is to insert a nasogastric tube to feed . However, the failure of this procedure will further confirm the diagnosis.
At the same time, the definitive diagnosis will still be thanks to imaging tools, especially x-ray with contrast. Thereby, the doctor will classify according to the morphology of congenital esophageal atrophy through the characteristics of the obturator bag, the distance of the two ends of the obturator bag as well as the presence and number of probes with the trachea.
However, congenital esophageal atrophy is often also identified before birth by fetal ultrasonography suggesting signs of fetal excess amniotic fluid or "absence stomach" sign.

Trẻ quấy khóc là dấu hiệu của teo thực quản bẩm sinh
4. How to treat children with congenital esophageal atresia?
Congenital esophageal atrophy is a defect that can be completely corrected with surgical intervention. The biggest concern is nutrition in the first days after birth to prepare optimal preoperative condition for the baby.
The child is exclusively fed parenteral nutrition. At the same time, the child should always be in a position of head height 30 to 40 degrees, good control of the child's airway, continuous suction of viscous sputum and saliva to minimize the possibility of aspiration, creating conditions for pneumonia and respiratory failure. aspiration, especially in the presence of tracheal fistula.
For any reason delaying surgery, a nasogastric tube is placed in the upper esophageal sphincter and suctioned through the catheter to reduce the risk of regurgitation through the tracheal fistula into the airway.
When the right time is reached and the infant's condition is stable, the doctor will perform surgery to connect the two ends of the esophagus. If a tracheal fistula is present, the fistula will also be ligated. In cases where the distance between the two ends of the esophagus is very long, the doctor will perform a gastric transposition procedure or use an autologous intestine to replace the missing part of the esophagus.

Phẫu thuật nối hai đầu thực quản là một phương pháp điều trị teo thực quản bẩm sinh
5. What to keep in mind when following up with congenital esophageal atrophy?
The most common acute complication of congenital esophageal atresia is a leak at the anastomosis site, which sometimes requires second-stage surgical repair.
Another very common difficulty that may be encountered in feeding infants, despite successful esophageal repair, is limited mobility of the distal esophagus. The incidence of this defect can be as high as 85% of cases. This is the reason why babies are very susceptible to acid reflux later in life.
In addition, in the process of taking care of children, it is necessary to pay attention to complications related to abnormalities in the esophagus that may occur, such as infants easily inhaling saliva and other liquids into the lungs, causing inflammation. lungs, wheezing, bronchospasm, respiratory failure and possibly death. At the same time, in the long term, it is necessary to pay attention to screen for the possibility of scarring of the esophageal stricture due to surgery or physiological esophageal stenosis as the child develops more physically.
Finally, because congenital esophageal atrophy is closely associated with other congenital malformations; Among them are deformities that can be resolved by surgery. Therefore, comprehensive screening for birth defects in terms of structural integrity and physiological function of organ systems is essential in the first days of life. This both helps to establish appropriate care for the child as well as helps guide a detailed and systematic plan of surgical intervention, avoiding the need for unexpected additional surgery.
In summary, infants born with congenital esophageal atrophy are a complex problem, not only because of the possibility of radical surgery, but also because of other related congenital malformations and long-term care after surgery. However, with good management and screening during pregnancy combined with advanced surgical techniques in neonates, these infants still have a very satisfactory long-term prognosis.
Before taking a job at Vinmec Central Park International General Hospital, the position of Doctor of Radiology since February 2018, Doctor Trinh Le Hong Minh used to work as a resident in the Department of Radiology. at hospitals: Cho Ray, University of Medicine and Pharmacy, Oncology, People's Gia Dinh, Trung Vuong... from 2012-2015. Working officially at Cho Ray Hospital from 2015-2016, City International Hospital since 2016.
To register for examination and treatment at Vinmec International General Hospital, you can contact Medical System Vinmec clinics nationwide, or register online HERE.
SEE MORE
Signs of children with congenital esophageal atrophy Surgery to treat esophageal atrophy Can this long-term esophageal stenosis be treated?